Downloaded 1,080 times



![Health education is a process which informs, motivate and
helps people to adopt and maintain healthy practices and life
styles; advocates environmental changes as needed to facilitate
this goal and conducts professional training and research to the
same end. - The National Conference on Preventive Medicine
[USA]
Health protection is the branch of public health concerned with
policies and practice to improve the prevention and control of
diseases and other environmental threats to the health of the
population.
Disease prevention covers measures not only to prevent the
occurrence of disease, such as risk factor reduction, but also to
arrest its progress and reduce its consequences once
established.](https://image.slidesharecdn.com/healthpromotion-introduction-170916082410/75/Health-Promotion-Introduction-7-2048.jpg)

































The document discusses the history and definitions of health promotion. It provides: 1) The term "health promotion" was first used in 1974 and refers to strategies that tackle the wider determinants of health beyond just healthcare. 2) Health promotion aims to empower people to have more control over their health and aspects of their lives that affect it. 3) Key strategies of health promotion include building healthy public policy, creating supportive environments, strengthening community action, developing personal skills, and reorienting health services.
Introduction of Col Zulfiquer Ahmed Amin with qualifications from Armed Forces Medical Institute.
Health Promotion first used by Marc Lalonde in 1974, addressing lifestyle, environment, healthcare and biology.
Health Promotion raises health status; it empowers individuals and communities to control their health.
WHO defines Health Promotion as enabling control over health through social and environmental interventions.
Combination of initiatives targeting determinants of health, requiring cooperation across sectors.
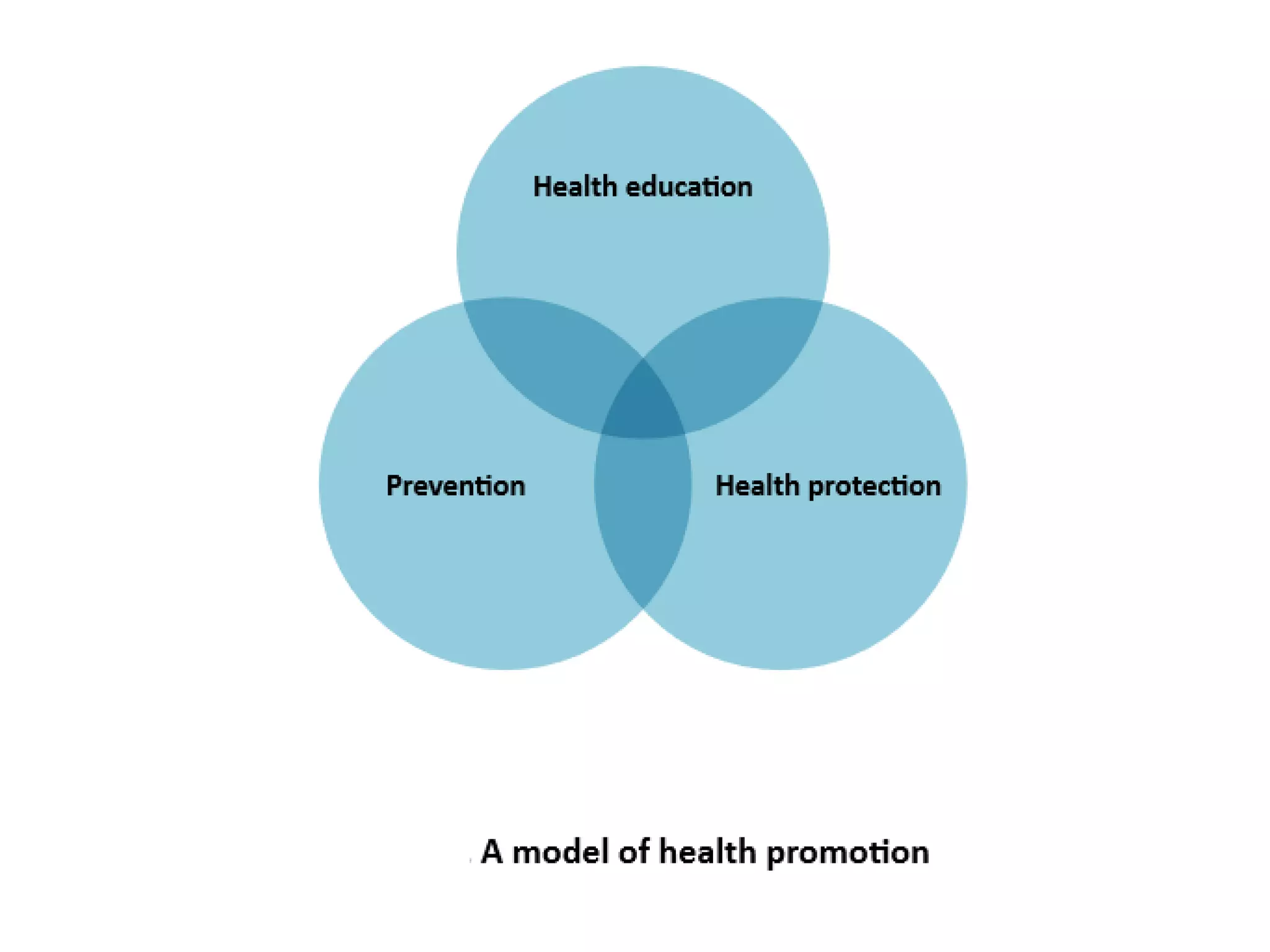
Health Education promotes healthy practices; Health Protection focuses on disease prevention and environmental safety.
Health Education informs behavior change, while Health Promotion focuses on social and environmental changes.
Health Promotion activities include education, preventative services, community mobilization, and policy implementation.
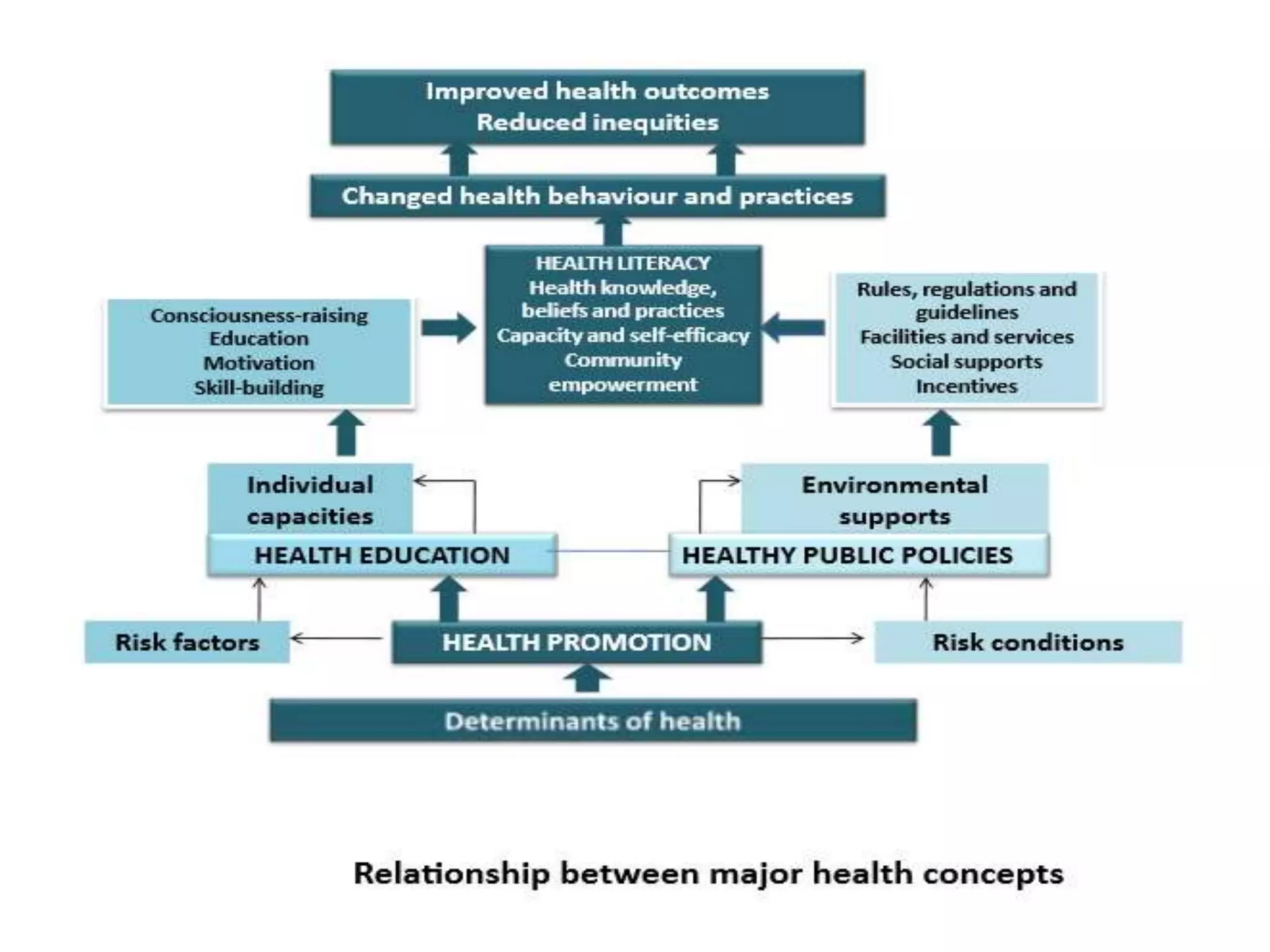
Health Promotion involves environmental action and is defined by the formula: Health Promotion = Health Education x Policy.
Cigarette warning labels exemplify successful health promotion impacting public policy and reducing risks.
Health Promotion enhances quality of life, reduces health inequalities, and is cost-effective.
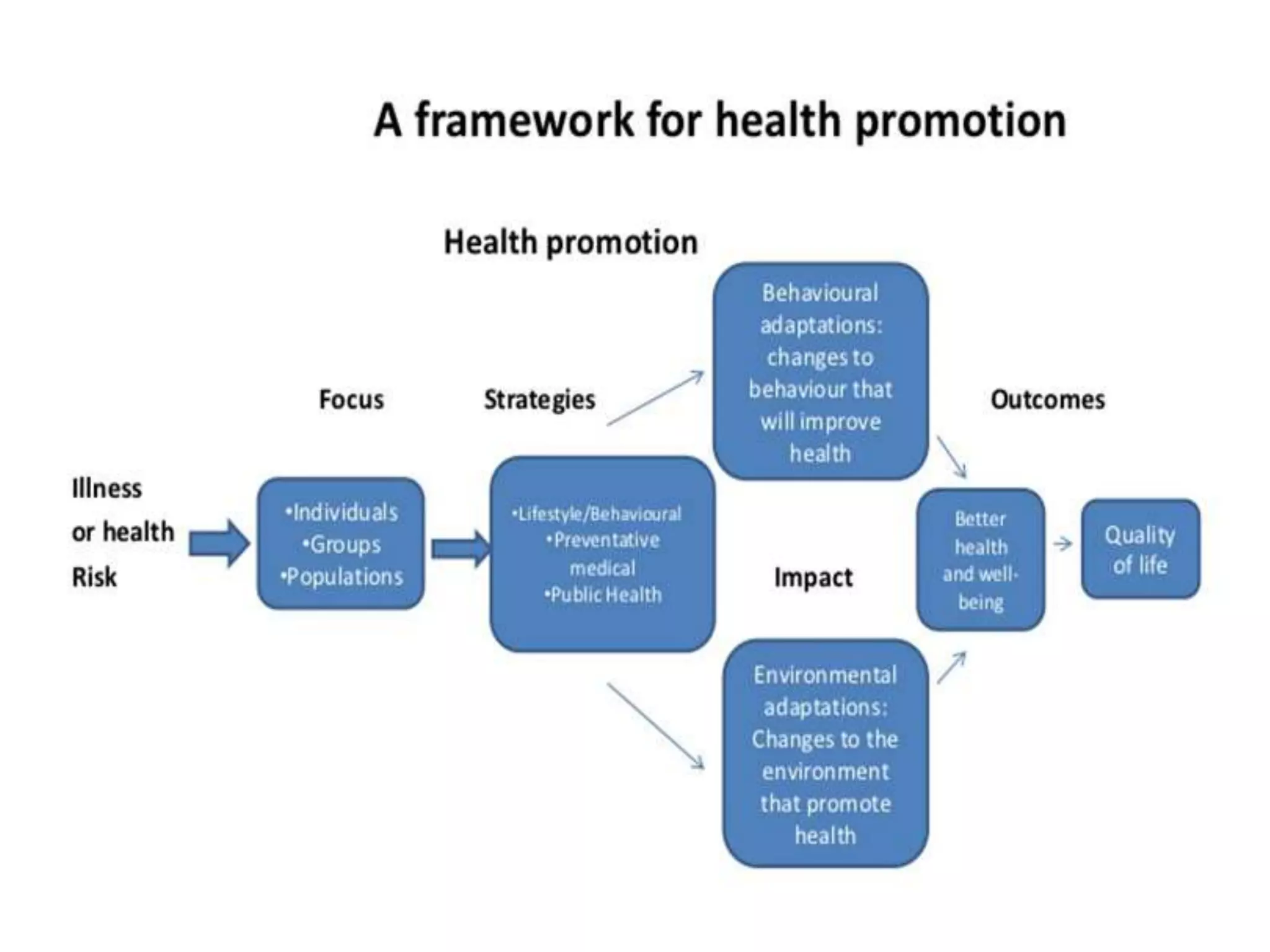
Focus, Strategies, Impact, Outcomes involving individuals and communities for better health quality.
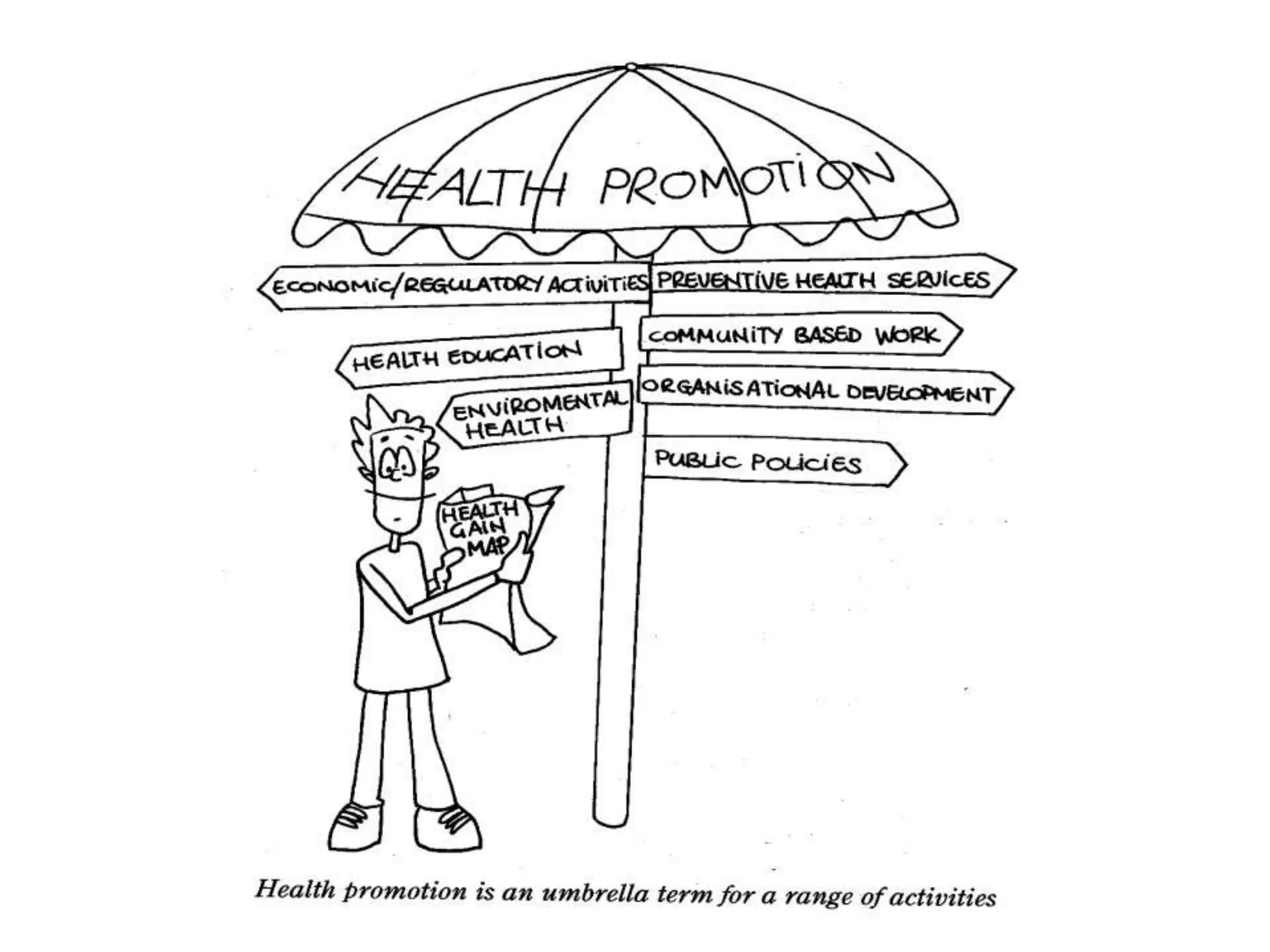
Areas of Health Promotion include preventive services, community work, organizational development, and more.
5 key principles include engaging the population, cooperative action on health determinants, and public participation.
Health Promotion combines communication, education, legislation, and community activities, being a societal endeavor.
List of significant Global Conferences on Health Promotion from 1986 to 2016 outlining priorities.
The Ottawa Charter outlines five areas for Health Promotion action: policy, environment, community action, skills, and services.
Identifies important areas like supportive environments, personal skills development, and healthy public policies.
Healthy Public Policy should predict health consequences and influence policies for health improvement.
Highlighting accountability and priority for health across policy areas to ensure health considerations.
Supportive environments enhance health by considering community needs, aiming for healthy living conditions.
Empowering communities actively to address health needs and ensuring their participation in health decisions.
Health Promotion provides skills and education for informed health decisions and life skill enhancement.
Focus shift from clinical services to health promotion, addressing determinants beyond just disease treatment.
Various non-health sectors like education, NGOs, and legal sectors contribute to health promotion efforts.
Health sectors such as nutrition and mental health play a significant role in promoting health.
Nine fundamental conditions for health improvements including peace, education, and social justice.
Three core strategies outlined: advocacy, enablement, mediation for effective health promotion.
Health promotion actions must ensure equitable health opportunities and resources for all individuals.
Health promotion requires collaboration across various sectors and groups for effective health improvement.
Advocacy involves influencing policy choices and promoting health access through community engagement.
Five identified approaches: Medical, Behaviour Change, Educational, Empowerment, and Social Change.
Focuses on reducing morbidity and preventing diseases through clinical interventions.
Emphasis on compliance, overlooks social factors, evaluates through disease rate reduction.
Targets individual behavior changes to reduce chronic conditions by promoting healthier actions.
Linked to health education, aiming to increase knowledge for informed health decisions.
Assumes knowledge leads to behavioral change, neglects social and economic constraints.
Focuses on helping individuals identify needs and gain skills for health self-management.
Distinguishes self-empowerment and community empowerment methods for health engagement.
Targets social and policy changes to improve population health through collective action.
Strategies include lobbying, creating supportive environments, and shaping health policies.
Explores five approaches used to tackle smoking and promote health.
Case study on integrating medical, behavioral, education, empowerment, and social strategies for smoking cessation.
Global health promotion recommendations focusing on women's health, hunger elimination, and supportive environments.
Emphasizes intertwining health and environmental issues for sustainable development.
Jakarta Declaration outlines five priorities to advance health promotion efforts globally.
Mexico Ministerial Statement emphasizes health as essential for life quality and socio-economic development.
Bangkok Charter calls for health promotion as a central responsibility in global development.
Final recap of the notable Global Health Promotion Conferences from 2009 to 2016.
Upcoming topics on models and history of health education and health promotion.























































































