Downloaded 12 times

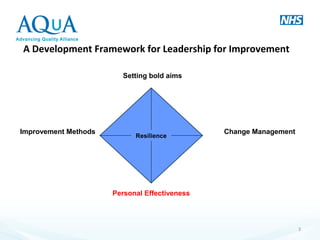
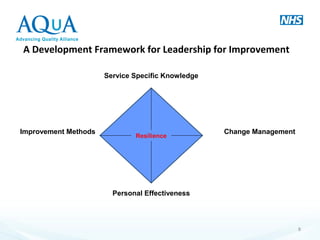

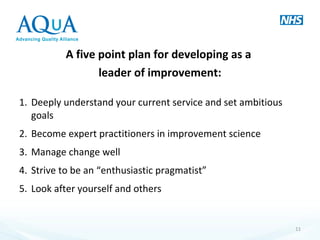

The document discusses a framework for leadership in change management within the NHS, emphasizing data-driven decision-making and the importance of engaged staff. It outlines a five-point plan for leaders to enhance their effectiveness and resilience while fostering a culture of improvement. Additionally, it highlights the need for reflective practices and collaboration to establish momentum in healthcare improvement initiatives.














































![What Your Employees Don't Know About Healthcare [Infographic]](https://cdn.slidesharecdn.com/ss_thumbnails/acainfographic-150909162847-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)