Download to read offline
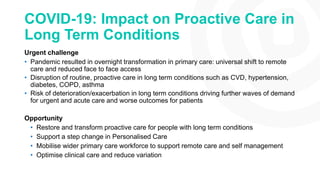

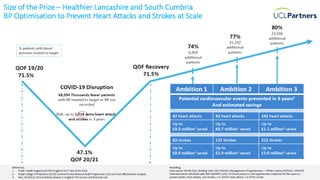
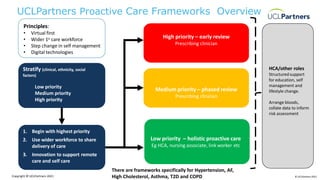
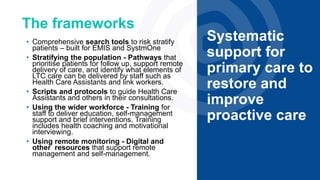
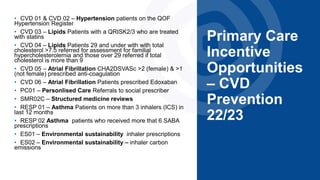

The document discusses the impact of the COVID-19 pandemic on proactive care in primary care, emphasizing the shift to remote care and the disruption faced in managing long-term conditions. It outlines a framework to restore proactive care, focusing on utilizing a wider primary care workforce, digital technologies, and support for self-management to improve patient outcomes. The document includes specific incentive opportunities for cardiovascular disease prevention and highlights the importance of personalized care and shared decision-making in addressing health inequalities.































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



