Downloaded 71 times


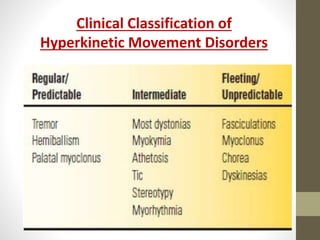
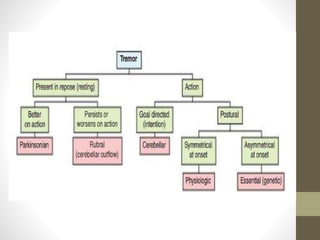
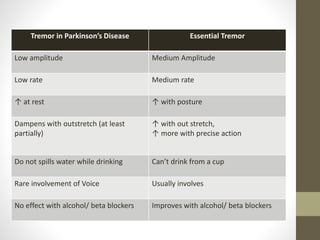
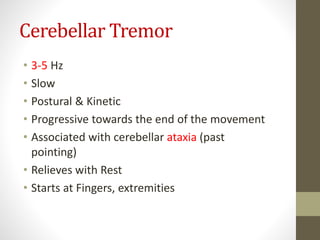
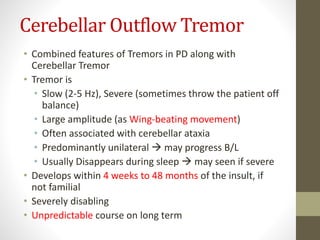
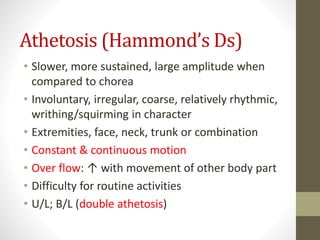
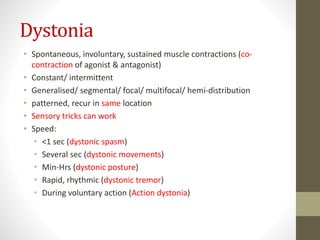

The document provides a comprehensive overview of hyperkinetic movement disorders, classifying them into various types such as tremors, chorea, dystonia, and myoclonus. It details the clinical examinations required to differentiate these disorders and their characteristics, such as amplitude, frequency, and patterns of movement. Additionally, information about associated conditions and examples of specific disorders is included.










































































