Hyperbaric oxygen therapy (HBOT) involves breathing 100% oxygen inside a pressurized chamber above sea level pressure. It has been used to treat various neurological conditions such as stroke and traumatic brain injury by reducing mitochondrial membrane permeability and reversing ischemia. However, the Undersea and Hyperbaric Medical Society currently only lists air/gas embolism and intracranial abscess as evidence-based indications, while research continues into other potential applications.

![DEFINITION
Hyperbaric oxygen therapy (HBOT) is
a treatment in which patients breathe 100% oxygen while inside
a hyperbaric chamber pressurized to greater than sea level (1 atmosphere absolute [ATA])
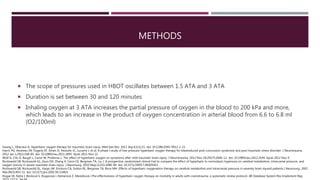
For clinical efficacy, the Undersea and Hyperbaric Medical Society specifies that the pressure must be
greater than or equal to 1.4 ATA
In clinical practice, pressures applied usually range from 2 to 3 ATA
Undersea and Hyperbaric Medical Society. Indications for hyperbaric oxygen therapy. https://www.uhms.org/resources/hbo-indications.html.
Thom SR. Hyperbaric oxygen: its mechanisms and efficacy. Plast Reconstr Surg 2011; 127(Suppl 1):131S-41S.](https://image.slidesharecdn.com/hyperbaricoxygentherapyforneurologicalconditions1118-181104084501/85/Hyperbaric-Oxygen-Therapy-for-Neurological-Conditions-2-320.jpg)