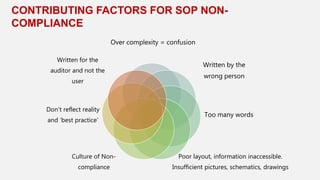
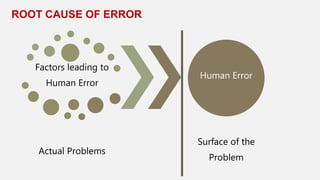
This document discusses human error and approaches to reducing it. It begins by defining human error as mistakes that cause accidents or bad outcomes. It then explores common causes of human error, including mental overload, poor work environments, habituated behaviors, poor understanding, and flawed decision making. Finally, it proposes solutions focused on simplification, such as better designed standard operating procedures, more precise practices, minimizing multi-tasking, addressing stress and ergonomics in the work environment, replacing bad habits through precise practice and feedback, and using fact-based and systematic approaches to decision making. The overall message is that human error can be reduced by simplifying systems and processes to better account for human limitations and behaviors.