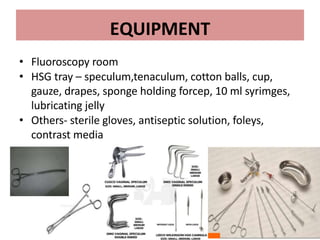
Hysterosalpingography is an imaging technique used to evaluate the uterus and fallopian tubes. It involves inserting a cannula through the cervix and injecting radiographic contrast material under fluoroscopy. This allows visualization of the uterine cavity, fallopian tubes and surrounding structures. The document discusses the indications, contraindications, procedure details, normal findings, and various pathologies that can be detected with hysterosalpingography such as uterine anomalies, tubal blockages, adhesions and infections.







![cotton-wool plug appearance
Distribution of contrast medium in a reticular pattern
producing a " cotton-wool plug" appearance [arrow]
73](https://image.slidesharecdn.com/hsg1ppt-240123153444-b1da5c34/85/HSG-1-PPT-pptx-73-320.jpg)
![BEADED TUBE
Multiple constrictions along the fallopian tube giving rise to
a " beaded" appearance [arrows]
74](https://image.slidesharecdn.com/hsg1ppt-240123153444-b1da5c34/85/HSG-1-PPT-pptx-74-320.jpg)
![LEOPARD SKIN APPEARANCE
Multiple rounded filling defects following intraluminal granuloma
formations within the hydrosalpinx, resembling a " leopard skin"
appearance [arrows]
78](https://image.slidesharecdn.com/hsg1ppt-240123153444-b1da5c34/85/HSG-1-PPT-pptx-78-320.jpg)
![CORK SCREW APPREANCE
Vertically fixed tubes secondary to dense peritubal
adhesions. Dense connective tissue causes the lack of tubal
mobility. The hyperconvulated right tube and manifests a "
cork screw" like appearance [arrows] 80](https://image.slidesharecdn.com/hsg1ppt-240123153444-b1da5c34/85/HSG-1-PPT-pptx-80-320.jpg)