Downloaded 20 times
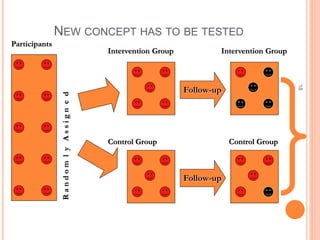
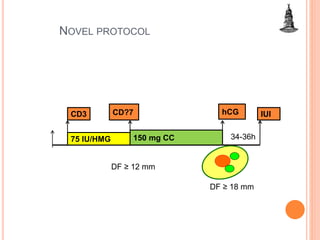
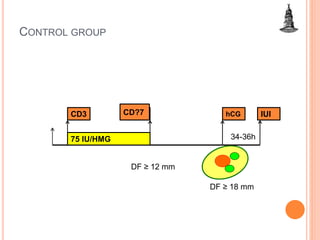
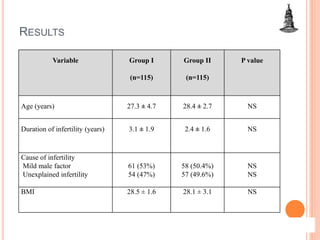
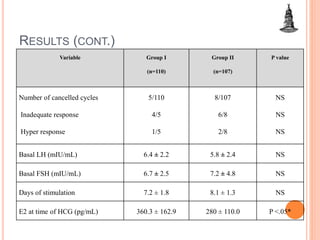
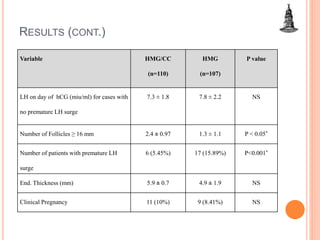
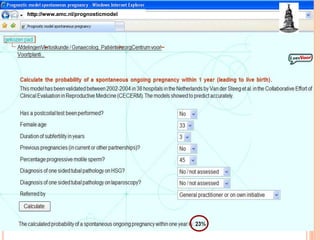
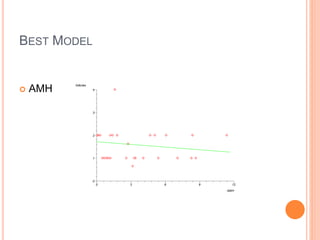
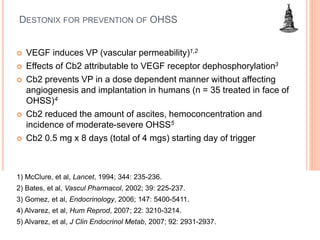
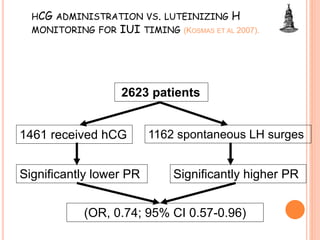

This document discusses how evidence-based medicine is changing attitudes in gynecologic practice. It provides an example of a randomized controlled trial comparing two ovarian induction protocols for intrauterine insemination. The trial found that using clomiphene citrate along with human menopausal gonadotropin reduced the rate of premature luteinizing hormone surges compared to human menopausal gonadotropin alone, with no significant differences in clinical pregnancy rates. The document outlines how evidence from randomized trials, prognostic models, economic analyses and other studies can inform clinical decision-making and change practices in gynecology.






































































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




