General management
Management of low grade gliomas: overview
Pilocytic astrocytoma
non pilocytic/diffuse infiltrating gliomas
Management of high grade gliomas: overview
Anaplastic gliomas
Glioblastoma multiformae
The treatment for sarcoma cancer is done only through the surgical methods in which the bone and soft-tissue of limb of the patient is saved from extremity tumour cases.
General management
Management of low grade gliomas: overview
Pilocytic astrocytoma
non pilocytic/diffuse infiltrating gliomas
Management of high grade gliomas: overview
Anaplastic gliomas
Glioblastoma multiformae
The treatment for sarcoma cancer is done only through the surgical methods in which the bone and soft-tissue of limb of the patient is saved from extremity tumour cases.
The 2016 World Health Organization classification of tumors of the central nervous system broadly employs genetic alterations for diagnostic criteria including isocitrate dehydrogenase-1 (IDH1) mutation or IDH2 mutation, and 1p/19q codeletion,[1] with the goal of creating more homogeneous disease categories with greater prognostic value.[2-5] Molecular diagnostics is becoming an increasingly important aspect of clinical oncologic neuropathology practice.
advancements in the diagnostics help detect states like oligometastasis ,which can lead to selection of patients for local and MDT and prolong the time to adjuvant therapy, at present There is no consensus on the treatment of oligometastatic cancer and clinical trials can help in evidence formation.
Stereotactic Radiotherapy of Recurrent Malignant Gliomas Clinical White PaperBrainlab
Learn more: https://www.brainlab.com/intraoperative-mri
Tumors of the central nervous system (CNS) represent approximately 176,000 newly diagnosed cases worldwide per year, with an estimated annual mortality of 128,000. Malignant gliomas comprise 30% of all primary CNS tumors and remain one of the greatest challenges in oncology today, despite access to state-of-the-art surgery, imaging, radiotherapy and chemotherapy.
GLIOBLASTOMA MULTIFORME
This seminar is presented as a part of weekly journal club and seminar regularly conducted at Apollo hospital,Kolkata Department of Radiation oncology.
This deals with novel molecular findings and their implications in Ewings sarcoma. The role of dose dense and dose intense chemotherapy and role of high dose chemotherapy. Additionally it also deals with survivor ship issues
Modeling the Dynamics of Glioblastoma Multiforme and Cancer Stem CellsStephen Steward
In this talk, we extend the work of Kronik, Kogan, Vainstein, and Agur (2008) by incorporating the cancer stem cell hypothesis into a treatment model for Glioblastoma Multiforme. Cancer Stem Cells (CSCs) are a specialized form of tumor cell with normal adult stem cell properties. CSCs are believed to be one of the primary reasons for cancer recurrence since they are more resilient to current treatment practices and are able to repopulate the tumor. We present a system of nonlinear ordinary differential equations that describes the interaction between cancer stem cells, tumor cells, and alloreactive cytotoxic-T-lymphocytes (CTLs). Under the assumption of constant treatment, we present conditions on the treatment amount that leads to a locally stable cure state. We also explore a more biologically accurate treatment schedule in which CTLs are injected periodically. In the case of periodic treatment, we numerically establish treatment schedules that lead to cancer persistence, cancer recurrence, and cancer eradication. We conclude with a sensitivity analysis of our parameters and a discussion of biological implications.
CCRT has:
1. Synergistic benefit against head and neck cancers
2. Associated with high level of response in in-operable disease
3. Tumour-radiosensitizing properties of chemotherapy or novel agents
4. Preservation of function is a major endpoint of interest
This study: efficacy of CCRT with a single agent
carboplatin in locally advanced head and neck cancers
The Influence of Transurethral Resection of Bladder Tumor on Staging of Bladd...asclepiuspdfs
Introduction: Bladder cancer is common, expensive, and the number of cases rising with increased survival in the elderly population. Most centers do computed tomography (CT) scan at the point of investigation, and some will carry this out along with magnetic resonance imaging (MRI) scan to have better local staging once the diagnosis of invasive cancer is made. Any surgical procedure would have a likelihood of influencing local staging, and this is a common belief without any evidence. Methods: We have retrospectively analyzed our data to see where the truth lies. We have compared the final pathology of 236 radical cystectomy patients to the staging reports of 241 CT scans and 65 MRI scans. Results: We have ascertained accuracy, sensitivity, and specificity and whether they were influenced by the timing of the transurethral resection of bladder tumor (TURBT). There was no significant difference between CT and MRI and the timing of the TURBT. Conclusion: This is the first report in the literature outlining the influence of TURBT. We accept the limitation due to the retrospective nature, small sample size, and variability of the biology of bladder cancer.
Secondary Malignancy after Treatment of Prostate Cancer. Radical Prostatectom...asclepiuspdfs
Background: This study aims to determine whether the treatment of locally confined prostate cancer (PCa) with external radiotherapy (EBRT) increases the risk to develop secondary malignancies (SM) compared to radical prostatectomy (RPE). Materials and Methods: Data from patients who were treated curatively with RPE or EBRT from 2010 to 2018 and who did not have distant metastases, previous malignancy, or previous treatment with radiotherapy or chemotherapy at the time of diagnosis were reviewed to determine the incidence of SM over a median follow-up period of 47 months (range 12–96 months). Regression models were used to correlate the clinicopathological factors with the incidence of SM.
This lecture proves an overview of assessing the thyrod nodule upon presentation. The use of imaging, including nuclear medicine, PET, CT/MR and Ultrasound is discussed.
There is more detail on ultrasound evaluation with particular emphasis on ACR TIRADS
Social Media en Woningpresentatie bij 't WooninvesteringsfondsJannetta Dorsman
Presentatie aan de verkopende makelaars van het Wooninvesteringsfonds (WIF) over Social Media en de makelaardij, Woningpresentatie en het verkopen van huizen. Workshop vond plaats op dinsdag 20 september in Zeist.
The 2016 World Health Organization classification of tumors of the central nervous system broadly employs genetic alterations for diagnostic criteria including isocitrate dehydrogenase-1 (IDH1) mutation or IDH2 mutation, and 1p/19q codeletion,[1] with the goal of creating more homogeneous disease categories with greater prognostic value.[2-5] Molecular diagnostics is becoming an increasingly important aspect of clinical oncologic neuropathology practice.
advancements in the diagnostics help detect states like oligometastasis ,which can lead to selection of patients for local and MDT and prolong the time to adjuvant therapy, at present There is no consensus on the treatment of oligometastatic cancer and clinical trials can help in evidence formation.
Stereotactic Radiotherapy of Recurrent Malignant Gliomas Clinical White PaperBrainlab
Learn more: https://www.brainlab.com/intraoperative-mri
Tumors of the central nervous system (CNS) represent approximately 176,000 newly diagnosed cases worldwide per year, with an estimated annual mortality of 128,000. Malignant gliomas comprise 30% of all primary CNS tumors and remain one of the greatest challenges in oncology today, despite access to state-of-the-art surgery, imaging, radiotherapy and chemotherapy.
GLIOBLASTOMA MULTIFORME
This seminar is presented as a part of weekly journal club and seminar regularly conducted at Apollo hospital,Kolkata Department of Radiation oncology.
This deals with novel molecular findings and their implications in Ewings sarcoma. The role of dose dense and dose intense chemotherapy and role of high dose chemotherapy. Additionally it also deals with survivor ship issues
Modeling the Dynamics of Glioblastoma Multiforme and Cancer Stem CellsStephen Steward
In this talk, we extend the work of Kronik, Kogan, Vainstein, and Agur (2008) by incorporating the cancer stem cell hypothesis into a treatment model for Glioblastoma Multiforme. Cancer Stem Cells (CSCs) are a specialized form of tumor cell with normal adult stem cell properties. CSCs are believed to be one of the primary reasons for cancer recurrence since they are more resilient to current treatment practices and are able to repopulate the tumor. We present a system of nonlinear ordinary differential equations that describes the interaction between cancer stem cells, tumor cells, and alloreactive cytotoxic-T-lymphocytes (CTLs). Under the assumption of constant treatment, we present conditions on the treatment amount that leads to a locally stable cure state. We also explore a more biologically accurate treatment schedule in which CTLs are injected periodically. In the case of periodic treatment, we numerically establish treatment schedules that lead to cancer persistence, cancer recurrence, and cancer eradication. We conclude with a sensitivity analysis of our parameters and a discussion of biological implications.
CCRT has:
1. Synergistic benefit against head and neck cancers
2. Associated with high level of response in in-operable disease
3. Tumour-radiosensitizing properties of chemotherapy or novel agents
4. Preservation of function is a major endpoint of interest
This study: efficacy of CCRT with a single agent
carboplatin in locally advanced head and neck cancers
The Influence of Transurethral Resection of Bladder Tumor on Staging of Bladd...asclepiuspdfs
Introduction: Bladder cancer is common, expensive, and the number of cases rising with increased survival in the elderly population. Most centers do computed tomography (CT) scan at the point of investigation, and some will carry this out along with magnetic resonance imaging (MRI) scan to have better local staging once the diagnosis of invasive cancer is made. Any surgical procedure would have a likelihood of influencing local staging, and this is a common belief without any evidence. Methods: We have retrospectively analyzed our data to see where the truth lies. We have compared the final pathology of 236 radical cystectomy patients to the staging reports of 241 CT scans and 65 MRI scans. Results: We have ascertained accuracy, sensitivity, and specificity and whether they were influenced by the timing of the transurethral resection of bladder tumor (TURBT). There was no significant difference between CT and MRI and the timing of the TURBT. Conclusion: This is the first report in the literature outlining the influence of TURBT. We accept the limitation due to the retrospective nature, small sample size, and variability of the biology of bladder cancer.
Secondary Malignancy after Treatment of Prostate Cancer. Radical Prostatectom...asclepiuspdfs
Background: This study aims to determine whether the treatment of locally confined prostate cancer (PCa) with external radiotherapy (EBRT) increases the risk to develop secondary malignancies (SM) compared to radical prostatectomy (RPE). Materials and Methods: Data from patients who were treated curatively with RPE or EBRT from 2010 to 2018 and who did not have distant metastases, previous malignancy, or previous treatment with radiotherapy or chemotherapy at the time of diagnosis were reviewed to determine the incidence of SM over a median follow-up period of 47 months (range 12–96 months). Regression models were used to correlate the clinicopathological factors with the incidence of SM.
This lecture proves an overview of assessing the thyrod nodule upon presentation. The use of imaging, including nuclear medicine, PET, CT/MR and Ultrasound is discussed.
There is more detail on ultrasound evaluation with particular emphasis on ACR TIRADS
Social Media en Woningpresentatie bij 't WooninvesteringsfondsJannetta Dorsman
Presentatie aan de verkopende makelaars van het Wooninvesteringsfonds (WIF) over Social Media en de makelaardij, Woningpresentatie en het verkopen van huizen. Workshop vond plaats op dinsdag 20 september in Zeist.
A different perspective on the Singularity Point . How IT is substituting job...Jacques Bulchand
A different perspective on the Singularity Point How IT is substituting jobs in the service sector.
Keynote at the 9th Multi Conference on. Computer Science. and Information Systems July 2015, Las Palmas, Spain
Ponencia impartida durante las I Jornadas COITIC de emprendimiento basado en las tecnologías organizada por el Colegio Oficial de Ingenieros Técnicos en Informática de Canarias
Sino-nasal cancers are not uncommon. However, treatment is always challenging because of surrounding critical normal structures.
Skilled surgical procedure and high end radiation therapy (IMRT, IGRT, SBRT) can definitely treat these difficult cancers.
Treatment of Brain Metastases Using the Current Predictive Models: Is the Pro...CrimsonpublishersCancer
Brain metastases from solid tumours are the most common intracranial tumours [1] and it occur in 40% of patients with cancer [2]. The most common primary tumours that metastasize to the brain are lung(40%),breast (25%) and melanoma (20%) [3]. The incidence is expected to be on the increase, due to improved survival, with use of modern cytotoxic drugs, targeted therapy, immunotherapy and modern radiotherapy techniques, in addition to greater use of magnetic resonance imaging of the brain. Brain metastases are common in the elderly, defined as above 60 years [4], and the interval between diagnosis of the primary and the development of brain metastases is variable, however some reported an average of 19 months [5] and adenocarcinoma is the commonest histology that metastasizes to the brain [6].
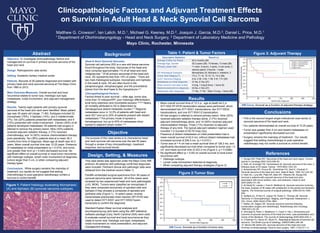
1. Figure 2:Tumor Size
KM Curve. Survival as a function of tumor size.
Clinicopathologic Factors and Adjuvant Treatment Effects
on Survival in Adult Head & Neck Synovial Cell Sarcoma
2013 Mayo Foundation for Medical Education and Research
Matthew G. Crowson1, Ian Lalich, M.D.1, Michael G. Keeney, M.D.2, Joaquin J. Garcia, M.D.2, Daniel L. Price, M.D.1
1 Department of Otorhinolaryngology - Head and Neck Surgery, 2 Department of Laboratory Medicine and Pathology
Mayo Clinic, Rochester, Minnesota
• This is the second largest single institutional case series of
synovial sarcoma of the head and neck.
• Our patients demonstrated an overall survival of 12.25 years.
• Tumor size greater than 4 cm and distant metastases on
presentation significantly decreased survival.
• Surgery remains the mainstay of treatment . Our results
suggest that adding chemotherapy to post-operative
radiotherapy may not confer a survival or control benefit.
Conclusions
1. Sturgis EM, Potter BO. Sarcomas of the head and neck region. Current
opinion in oncology.2003;15(3):239–52.
2. Roth JA, Enzinger FM, Tannenbaum M. Synovial sarcoma of the neck: a
followup study of 24 cases. Cancer. 1975;35(4):1243–53.
3. Bukachevsky RP, Pincus RL, Shechtman FG, Sarti E, Chodosh P.
Synovial sarcoma of the head and neck. Head & Neck. 1992;14(1):44–48.
4. Harb WJ, Luna MA, Patel SR, Ballo MT, Roberts DB, Sturgis EM.
Survival in patients with synovial sarcoma of the head and neck:
association with tumor location, size, and extension. Head & neck.
2007;29(8):731–40.
5. Al-Daraji W, Lasota J, Foss R, Miettinen M. Synovial sarcoma involving
the head: analysis of 36 cases with predilection to the parotid and temporal
regions. The American journal of surgical pathology. 2009;33(10):1494–
503.
6. Spillane AJ, A’Hern R, Judson IR, Fisher C, Thomas JM. Synovial
Sarcoma: A Clinicopathologic, Staging, and Prognostic Assessment. J.
Clin. Oncol. 2000;18(22):3794–3803..
7. Mullen JR, Zagars GK. Synovial sarcoma outcome following
conservation surgery and radiotherapy. Radiotherapy and Oncology.
1994;33(1):23–30.
8. Simunjak B, Petric V, Bedekovic V, Cupić H, Hat J. Dimensions and
outcome of synovial sarcoma of the head and neck: case presentation and
review of the literature. The Journal of otolaryngology.2005;34(6):420–3.
9. O’Sullivan PJ, Harris AC, Munk PL. Radiological features of synovial cell
sarcoma. The British journal of radiology. 2008;81(964):346–56.
10. Moore DM, Berke GS. Synovial sarcoma of the head and neck.
Archives of otolaryngology--head & neck surgery. 1987;113(3):311–3.
References
Objective. To investigate clinicopathologic factors and
management on survival in primary synovial sarcoma of the
head and neck.
Design. Retrospective case series.
Setting. Academic tertiary medical center.
Patients. Records of 28 patients diagnosed and treated with
primary head and neck synovial sarcoma at The Mayo Clinic
from 1960 to 2012.
Main Outcome Measures. Overall survival and local
recurrence related to tumor size, histologic sub-type,
metastases, nodal involvement, and adjuvant management
strategy.
Results. Twenty-eight patients with primary synovial
sarcoma of the head and neck were identified. Mean patient
age was 35 years old (range, 11-80). Subtypes included 22
monophasic (79%), 4 biphasic (14%), and 2 indeterminate
(7%). Six (22%) patients presented with metastases, and 4
(15%) presented with nodal involvement. Eleven (39%) of all
patients developed metastases. All patients had surgery in
attempt to remove the primary lesion. Nine (32%) patients
received adjuvant radiation therapy, 2 (7%) received
chemotherapy, and 14 (50%) receive chemoradiation therapy
post-operatively. Ten (36%) patients died at a mean 38.3
months from time of diagnosis. Mean age at death was 44.2
years. Mean overall survival time was 12.25 years. Presence
of metastases on initial presentation (p = 0.015), and tumor
size greater than 4cm (p = 0.040) decreased survival. No
significant effect on overall survival or local tumor recurrence
with histologic subtype, lymph node involvement at diagnosis,
tumors larger than 5 cm, or when comparing adjuvant
therapy types.
Conclusions. While surgery remains the mainstay of
treatment, our results do not suggest that adding
chemotherapy to post-operative radiotherapy confers a
survival or control benefit.
Abstract
Head & Neck Synovial Sarcoma:
Synovial cell sarcoma (SS) is a rare soft tissue sarcoma
found throughout the body. Sarcomas of the head and
neck comprise approximately 1% of all head and neck
malignancies.1 Of all primary sarcomas of the head and
neck, SS represents less than 10% of cases.1 There are
two main histological subtypes: monophasic and biphasic.
In the head & neck, SS are often found in the
parapharyngeal, retropharyngeal, and the prevertebral
planes from the skull base to the hypopharynx.2,3
Clincopathological Factors:
Factors linked to poor survival – older age, tumor size,
more than 10 mitoses/HPF, poor histologic differentiation,
local bony extension and incomplete excision.3,4,5,6 Nearly
all mortality attributed to SS is determined by
hematogenous distant metastatic burden.4,7 Regional
metastases occur in 12.5% of patients with head and
neck SS,8 and up to 25% of patients present with distant
metastases.9 The primary mode of spread is
hematogenous, but up to 20% of metastases show
spread to adjacent lymph nodes.2,10
Background
• Mean overall survival time of 12.3 yr., age at death 44.2 yr.
• SYT-SSX RT-PCR translocation assays were performed, which
demonstrated two SYT-SSX1 translocations, two SYT-SSX2
translocations, and one SYT-SSX1/2 translocation.
• All had surgery in attempt to remove primary lesion. Nine (32%)
received adjuvant radiation therapy alone, 2 (7%) received
adjuvant chemotherapy alone, and 14 (50%) received adjuvant
chemoradiation therapy. Three (11%) received no adjuvant
therapy of any kind. The typical adjuvant radiation regimen used
included 1-2 courses of 50-70 Gray (Gy).
• Presence of distant metastases on initial presentation had a
mean overall survival of 42.0 mo, without distant metastases had
increased survival of 206.5 mo. (p = 0.0151).
• Tumor size of > 4 cm had a mean survival time of 128.2 mo, and
significantly decreased survival when compared to tumor size < 4
cm and mean survival time of 223.2 mo (Figure 2, p = 0.0396).
• No significant effect (p > 0.05) on overall survival or local tumor
recurrence with:
• Histologic subtype.
• Lymph node involvement detected at diagnosis.
• When comparing adjuvant therapy strategies (Figure 3).
Results
The purpose of this case series is to characterize head
and neck synovial cell sarcoma over the last 50 years
through a review of key clinicopathologic, treatment
response, and survival trends.
Objective
This case series was approved under the Mayo Clinic IRB
protocol. All patients with pathology-confirmed diagnoses
were included. Pertinent clinical and pathologic data were
obtained from the medical record (Table 1).
Paraffin-embedded surgical specimens from 36 cases of
synovial sarcoma were retrieved. All of the cases were
reviewed by two experienced head and neck pathologists
(JJG, MGK). Tumors were classified as monophasic if
they were composed exclusively of spindled cells and
biphasic if they showed a composite of spindled and
epithelial cells (Figure 1). In select cases, reverse
transcriptase-polymerase chain reaction (RT-PCR) was
used to detect SYT-SSX1 and SYT-SSX2 fusion
transcripts to confirm the diagnosis.
Standard Kaplan-Meier survival analyses and
accompanying log-rank tests using the JMP statistical
software package (Cary, North Carolina USA) were used
to evaluate overall survival and local recurrence as they
relate to tumor size, histologic sub-type, metastases,
nodal involvement on initial presentation, and adjuvant
management strategy.
Design, Setting, & Measures
Table 1: Patient & Tumor Factors Figure 3: Adjuvant Therapy
KM Curve. Survival as a function of adjuvant therapy strategy.
Descriptive Statistics Result (n)
Average Follow-Up Period 83.4 months (26)
Average Age; Gender 35.3 years (28); 15 female, 13 male (28)
Primary Lesion Site 11 neck, 5 larynx, 4 spine, 3 oral cavity, 2
salivary gland, 2 thyroid, 1 scalp
SS Histological Subtypes Monophasic 22, Biphasic 4, Indeterm. 2
Tumor Size Staging (T) TX 2, T1 16, T2 10, T3, T4 0 (28)
AJCC Sarcoma Staging 9 IA, 2 IB, 3 IIA, 1 IIB, 5 III, 7 IV (28)
Metastases on initial diagnosis 21 No, 6 Yes (27)
Most common met sites (initial) 4 lung, 1 lung & bone, 1 bone (6)
Nodal involvement on diagnosis 23 No, 4 Yes (27)
Metastases after diagnoses 11 Yes, 17 No . Sites 10 lung, 1 bone (28)
Figure 1: Patient histology illustrating Monophasic
(A) and biphasic (B) synovial sarcoma subtypes.