Download as PDF, PPTX




![59
What Is HL7 CDA?
• “A document markup standard that
specifies structure & semantics of “clinical
documents” for the purpose of exchange”
[Source: HL7 CDA Release 2]
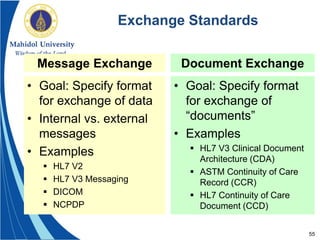
• Focuses on document exchange, not
message exchange
• A document is packaged in a message
during exchange
• Note: CDA is not designed for document
storage. Only for exchange!!](https://image.slidesharecdn.com/hl7standards-160914182058/85/Hl7-Standards-September-15-2016-59-320.jpg)


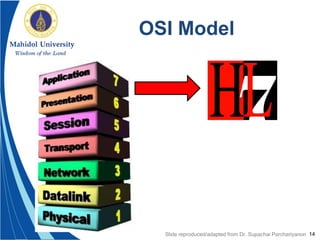
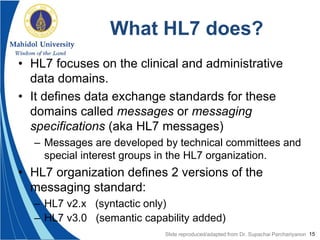
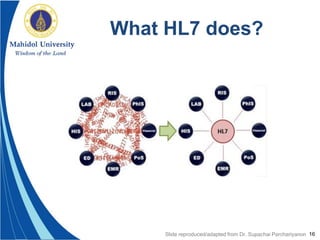
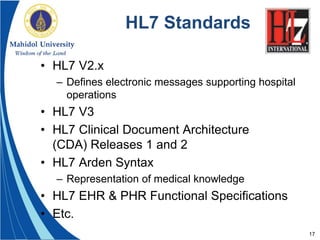
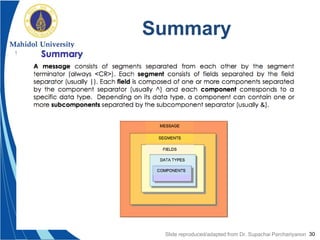
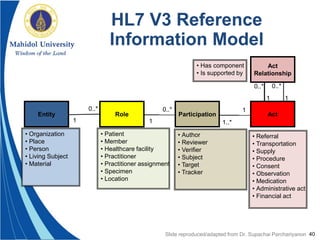
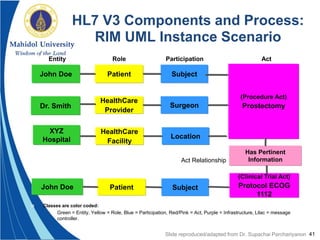
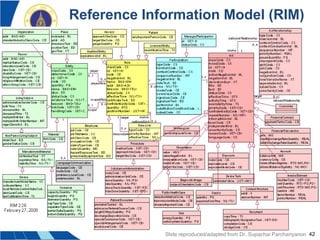
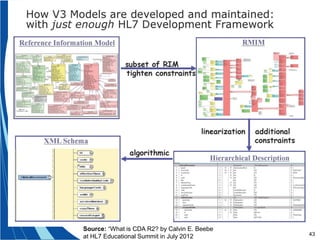
The document provides an overview of HL7 standards, focusing on interoperability in healthcare data exchange. It details the evolution from HL7 version 2, which is widely used in U.S. hospitals, to HL7 version 3, which aims to address limitations in v2 by incorporating a reference information model and using XML for messaging. The document also highlights future directions for HL7, including the introduction of FHIR for better resource management in clinical settings.