Downloaded 56 times

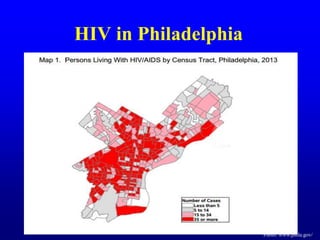
![Total: 35.0 million [33.2 million – 37.2 million]
Middle East & North Africa
230 000
[160 000 – 330 000]
Sub-Saharan Africa
24.7 million
[23.5 million – 26.1 million]
Eastern Europe &
Central Asia
1.1 million
[980 000– 1.3 million]
Asia and the Pacific
4.8 million
[4.1 million – 5.5 million]
North America and Western and Central Europe
2.3 million
[2.0 million – 3.0 million]
Latin America
1.6 million
[1.4 million – 2.1 million]
Caribbean
250 000
[230 000 – 280 000]
Adults and children estimated to be living with HIV2013](https://image.slidesharecdn.com/hivplanningcouncil2015-160201163610/85/HIV-Treatment-and-PrEP-in-2015-3-320.jpg)

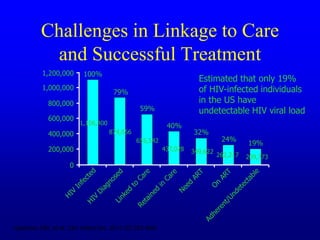

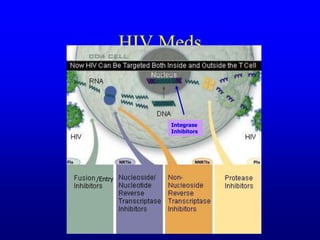

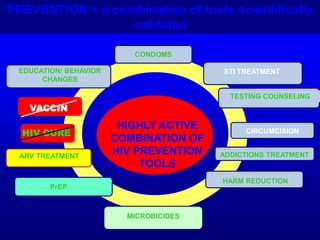
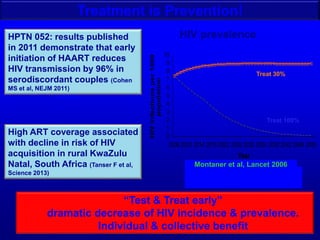


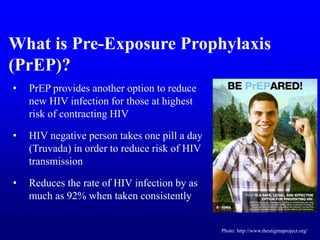







HIV treatment and PrEP options have advanced significantly since 2015. Key points: 1) Treatment as prevention is now recommended, with antiretroviral therapy shown to reduce HIV transmission by 96% and dramatically lower prevalence over time if treatment is scaled up. 2) PrEP using daily oral Truvada was found to reduce HIV risk by up to 92% in multiple studies when taken consistently, though adherence is important. Intermittent or on-demand PrEP was also found highly effective in some populations. 3) Several real-world demonstration projects confirmed PrEP's effectiveness in different settings and populations, with up to 86% reduced risk of HIV acquisition when PrEP was provided.



































































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)

