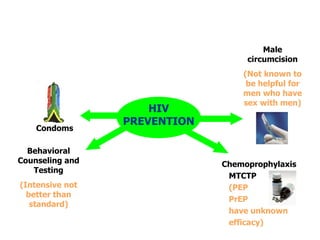
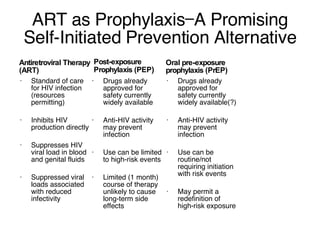
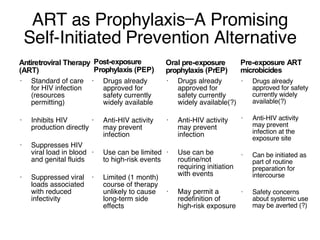
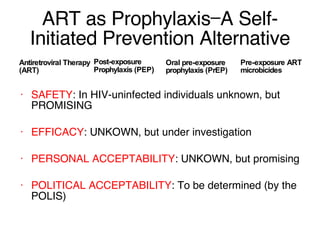
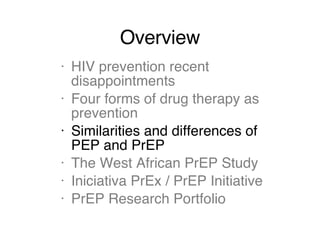
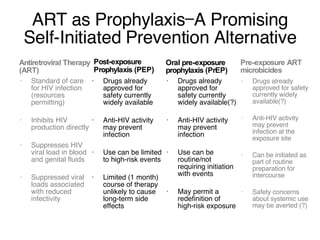
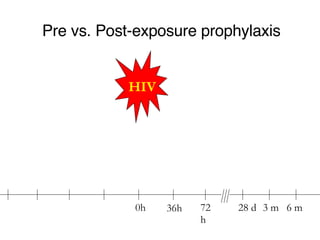
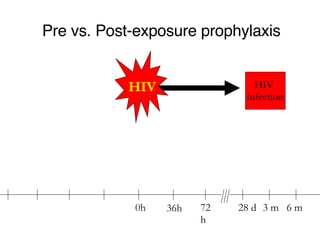
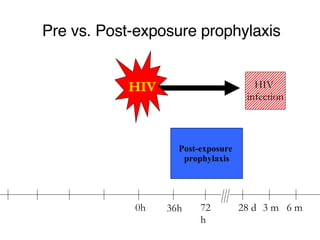
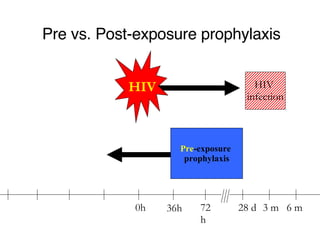
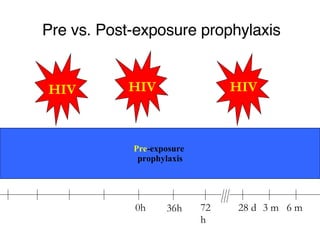
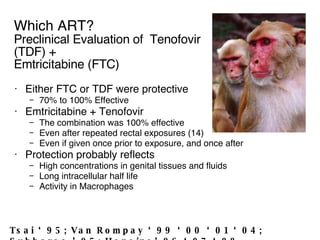
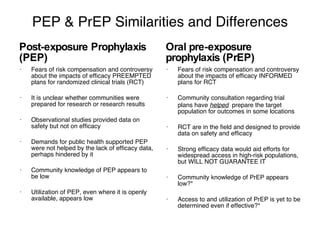
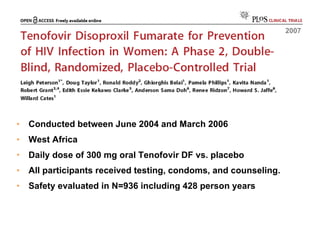
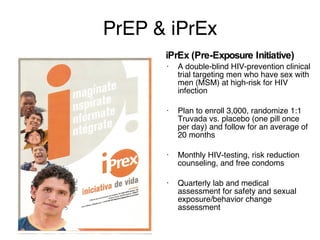
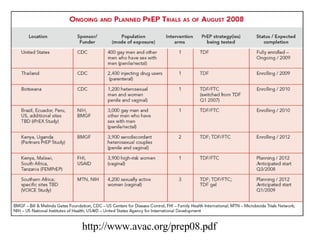
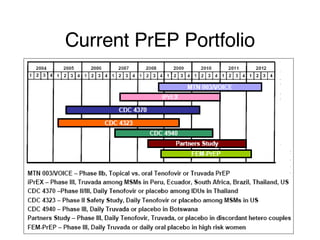
The document discusses various forms of drug therapy for HIV prevention, including post-exposure prophylaxis (PEP) and pre-exposure prophylaxis (PrEP), highlighting their similarities, differences, and effectiveness. It also reviews recent disappointments in HIV prevention trials, ongoing research studies, and the potential of antiretroviral therapy as a preventative measure. Key studies mentioned include the West African PrEP study and the iPrEx trial, both assessing safety and efficacy in high-risk populations.