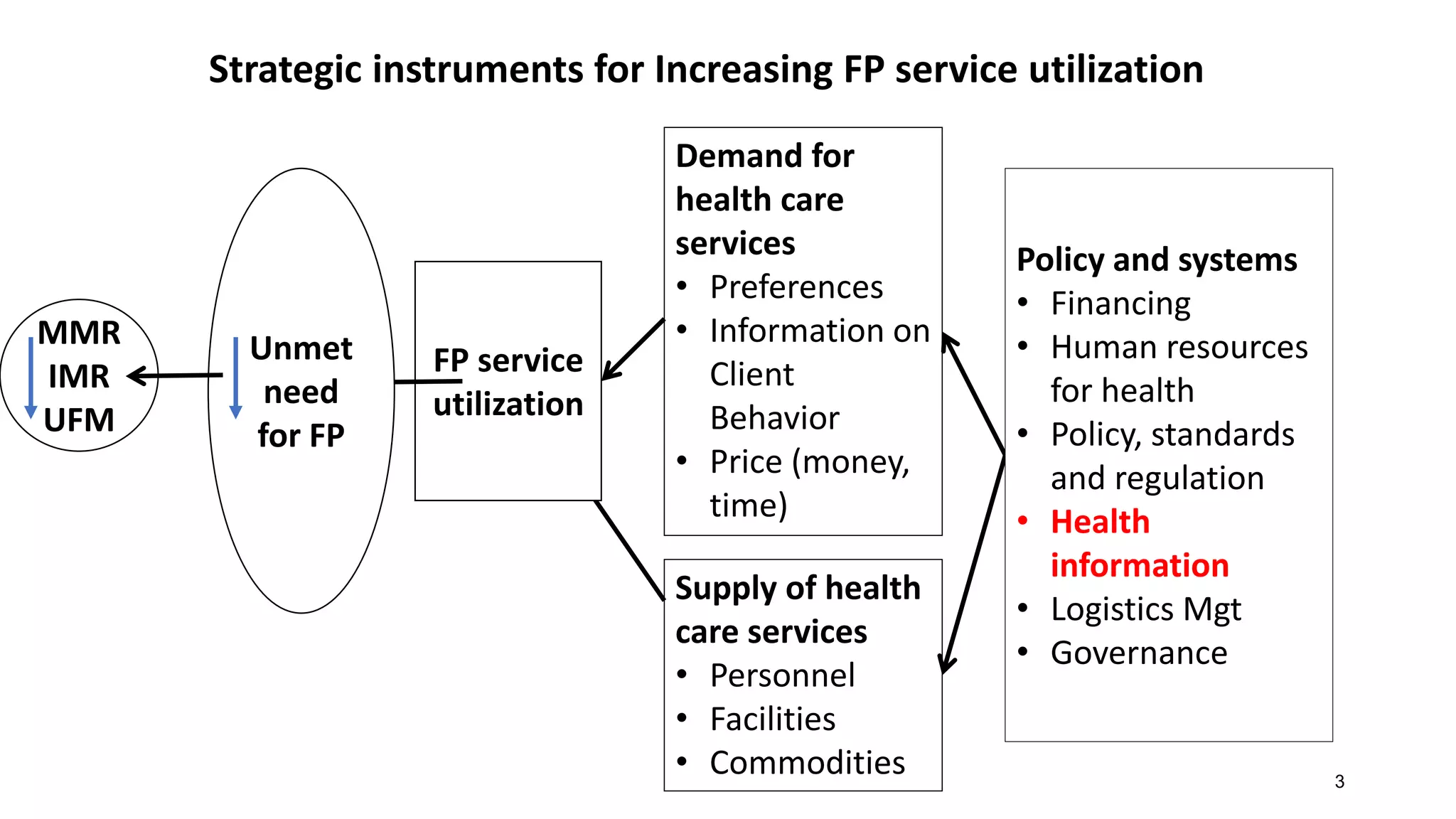
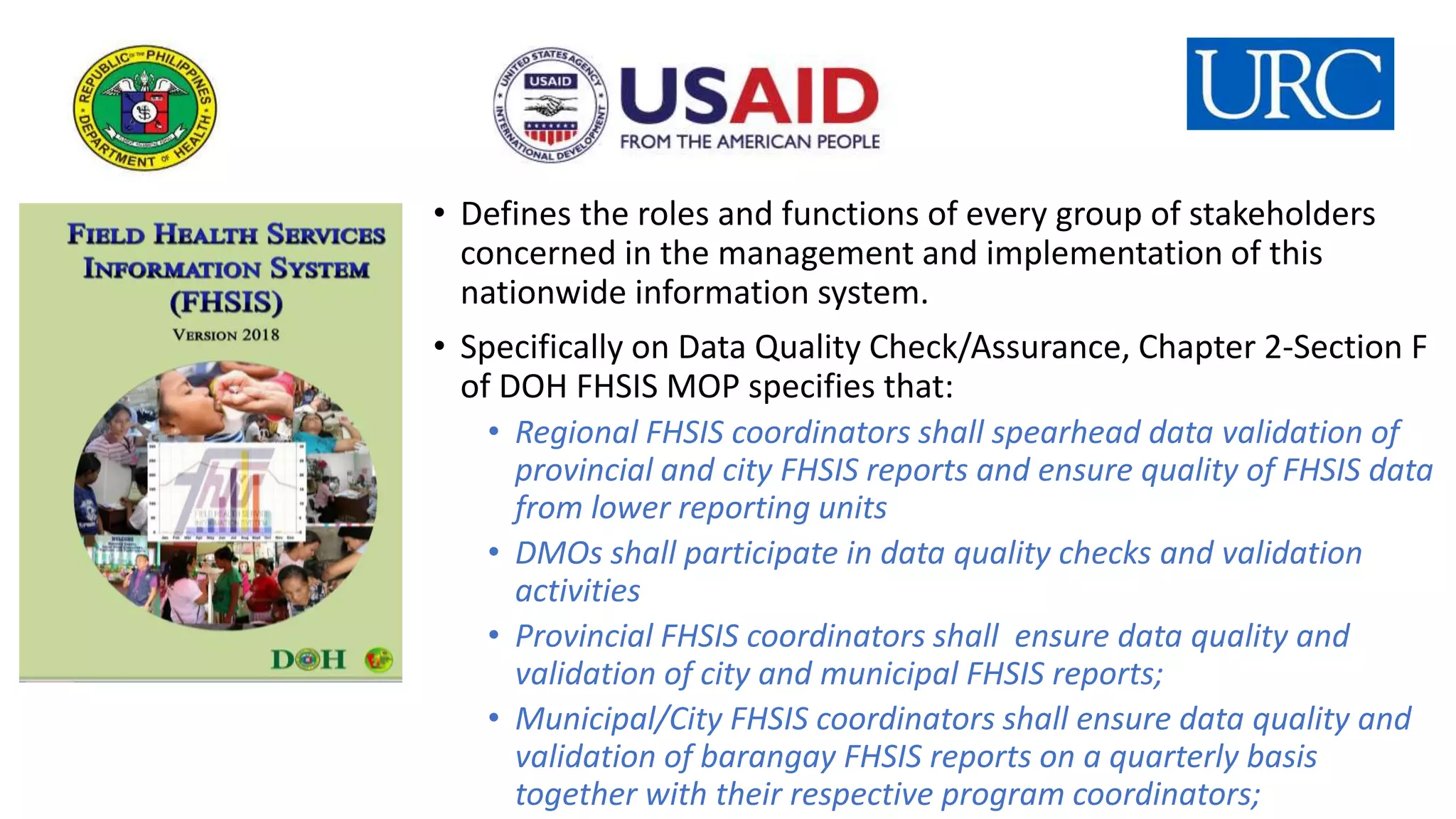
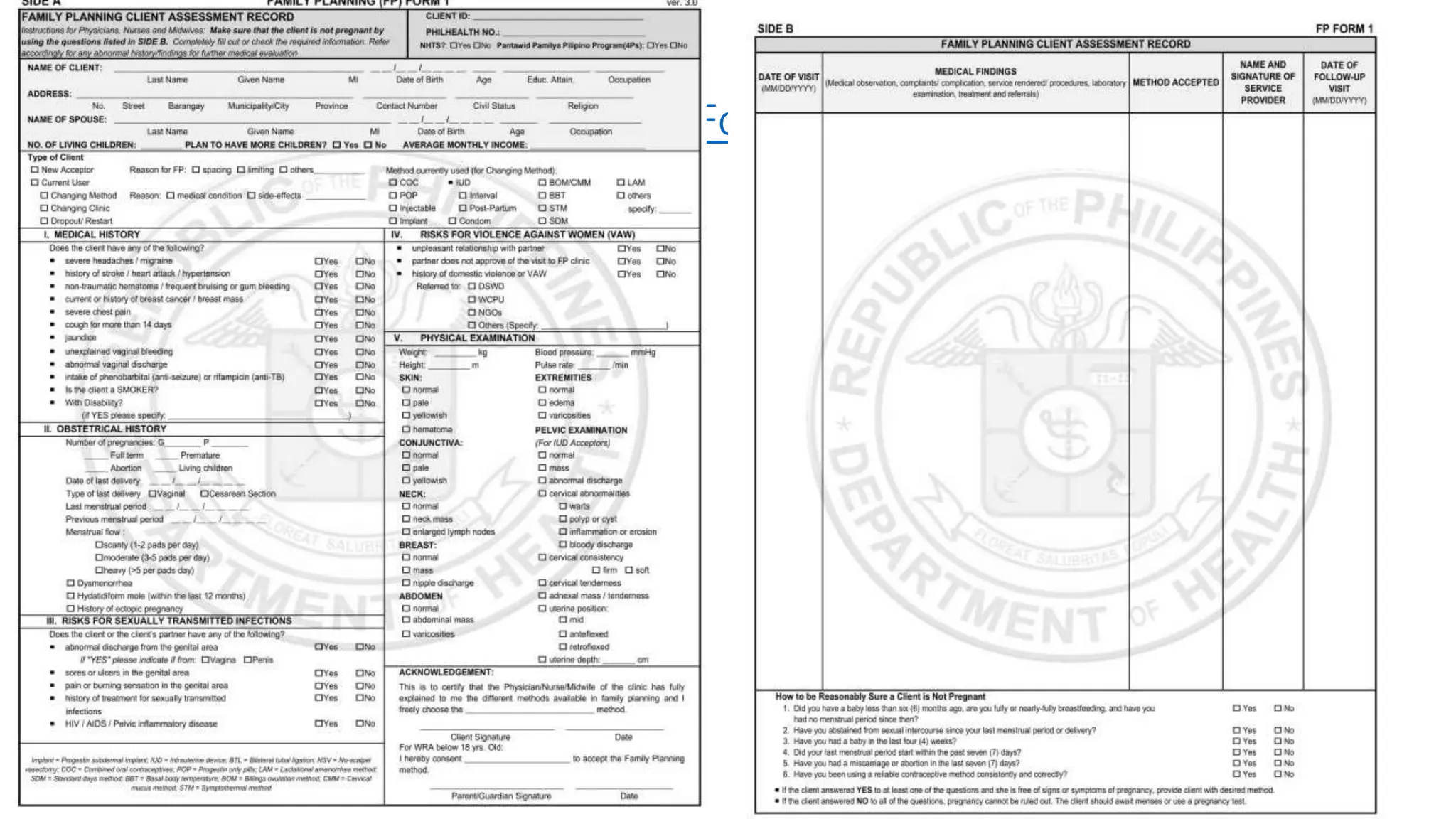
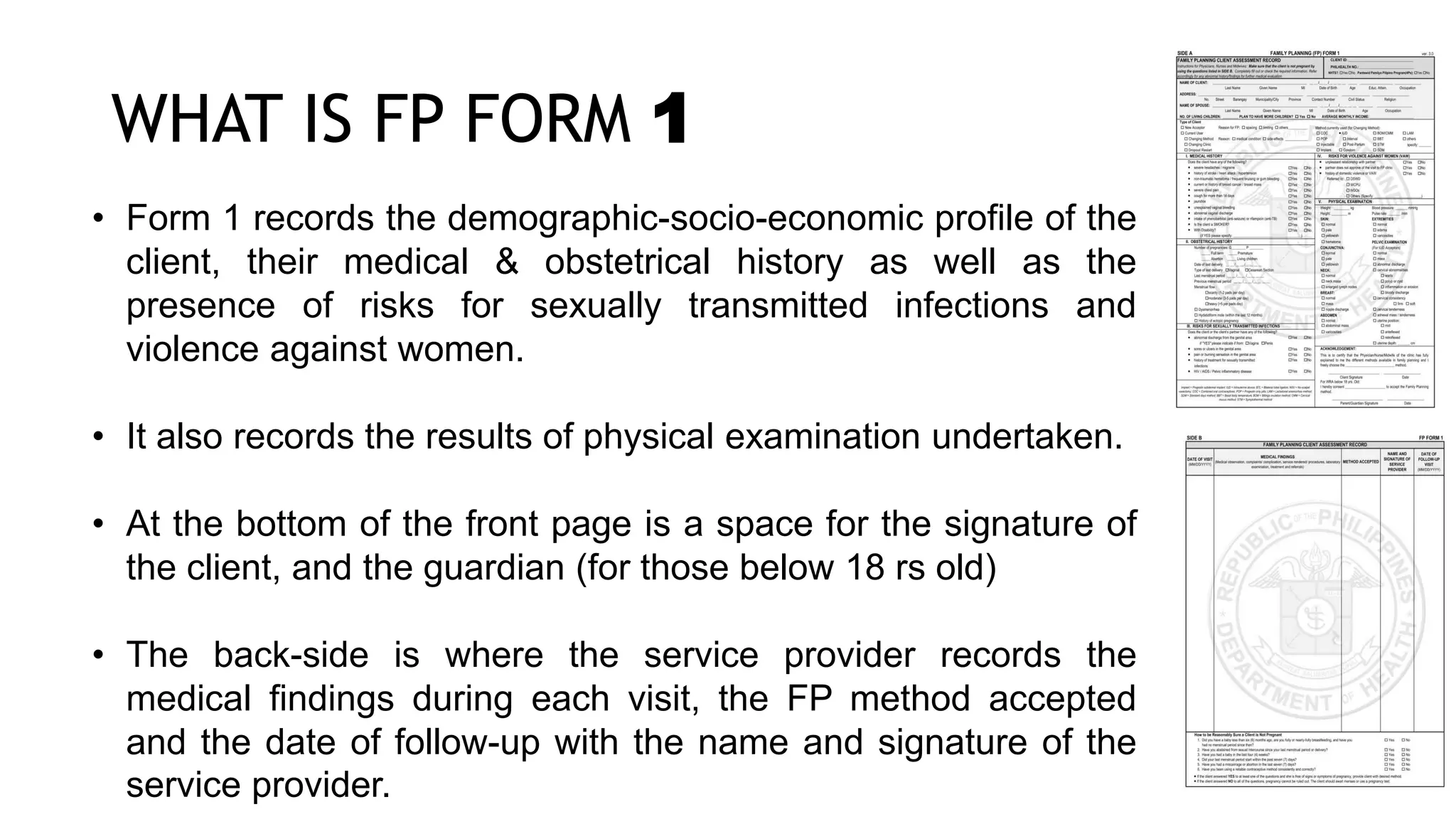
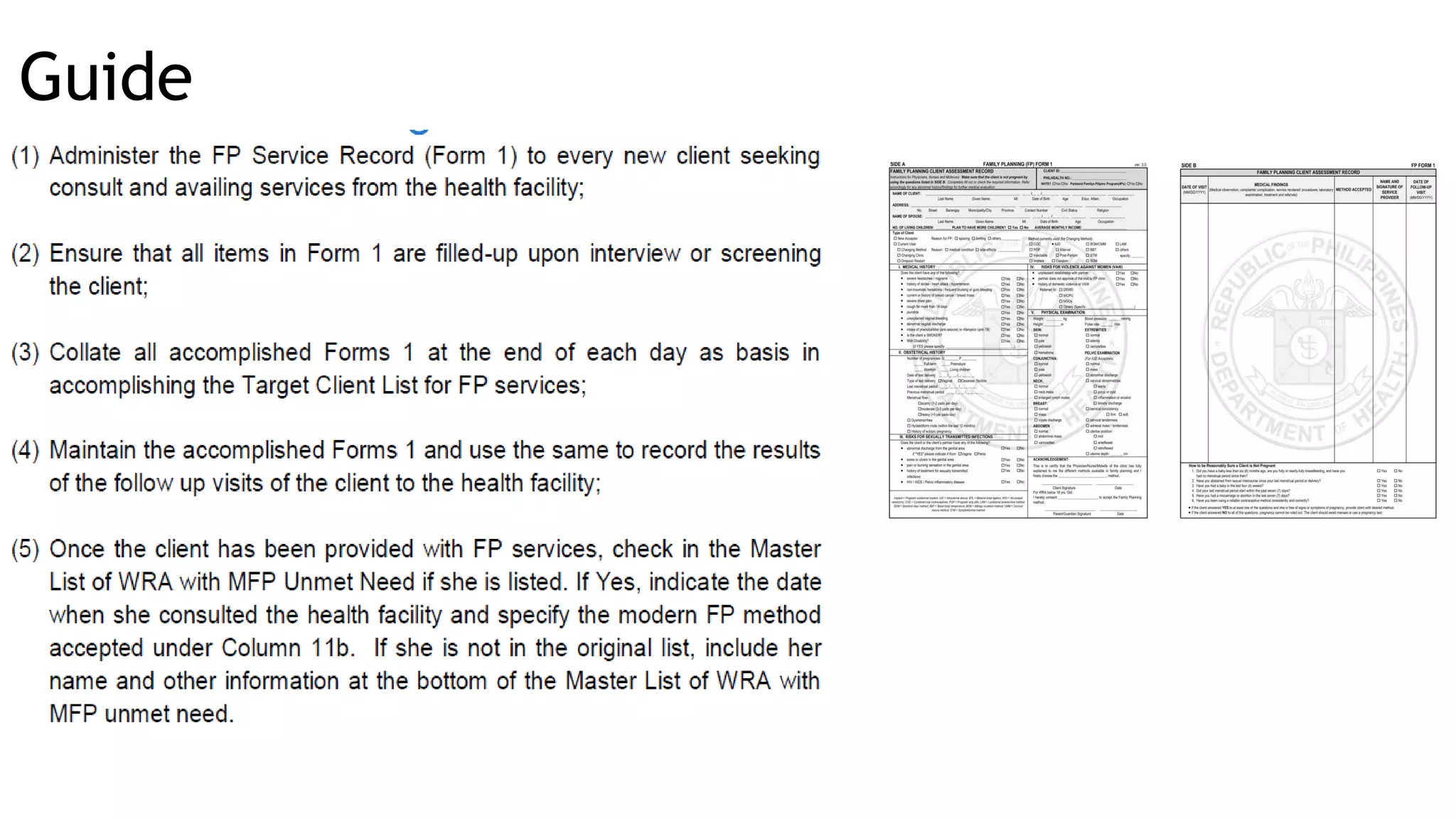
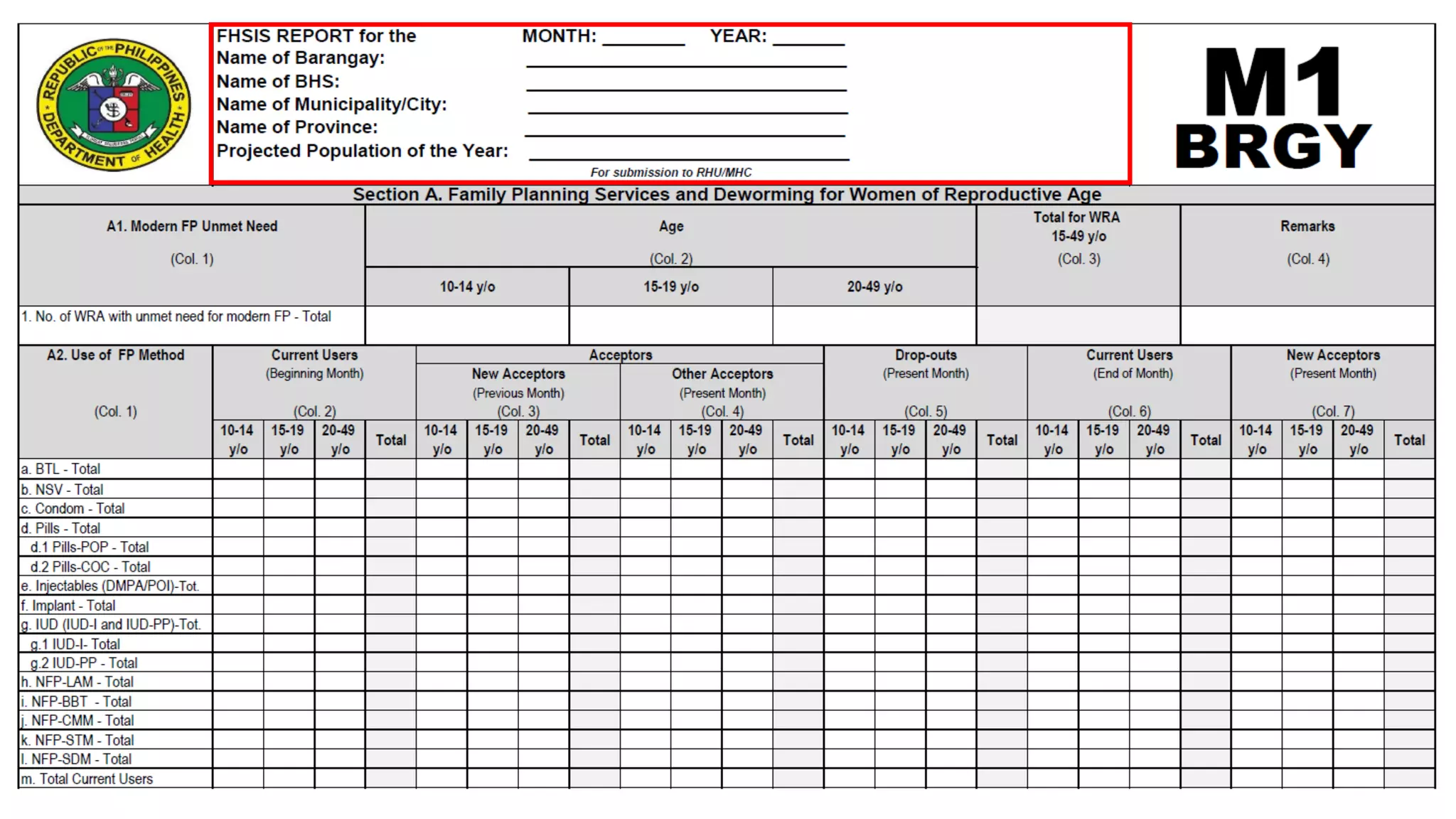
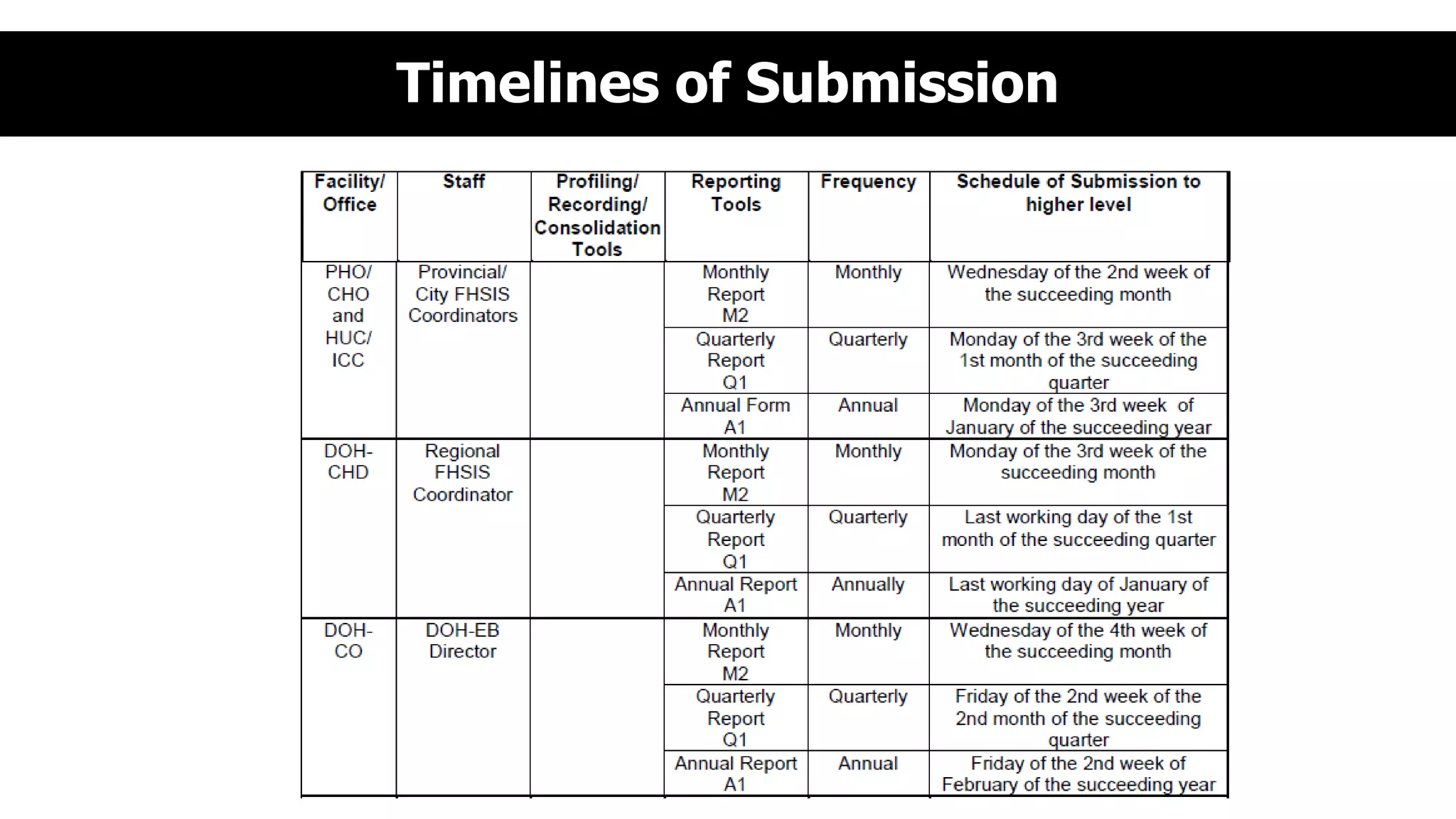
This document provides an overview and guidelines for training health workers on data quality checks for family planning data collected through the Field Health Service Information System (FHSIS) in BARMM. It discusses the FHSIS framework, key family planning forms used for recording service data at various levels of the health system, and rules for accurate reporting and drop-out tracking. Ensuring health workers have the skills and understanding needed to collect and report reliable family planning data is important for effective planning, resource allocation, and improving health outcomes in the region.
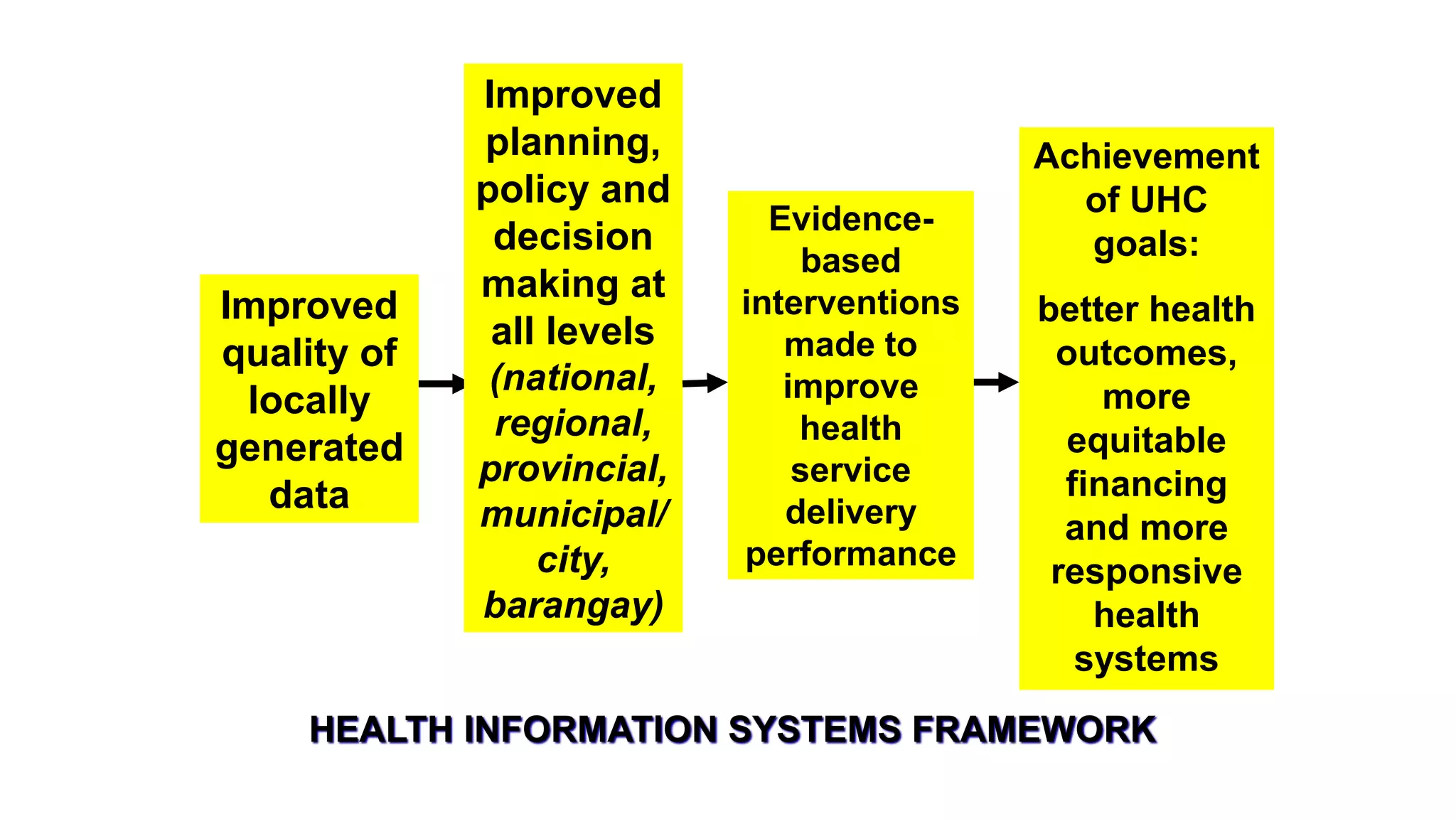
















![1. Determine the Current Users Beginning of Month by FP method and by Age
Group (10-14, 15-19, 20-49) [This is equivalent to Current Users End of
Previous Month] or copy Column 6 from M1 of Previous Month
2. Determine the number New Acceptors of the Previous Month by FP method
and by Age Group (10-14, 15-19, 20-49) or copy Column 7 from M1 of
Previous Month
3. Determine the number New Acceptors of the Present Month by FP method and
by Age Group (10-14, 15-19, 20-49) [TCL: refer to date of registration and
Type of Client is NA] and reflect under Column 7
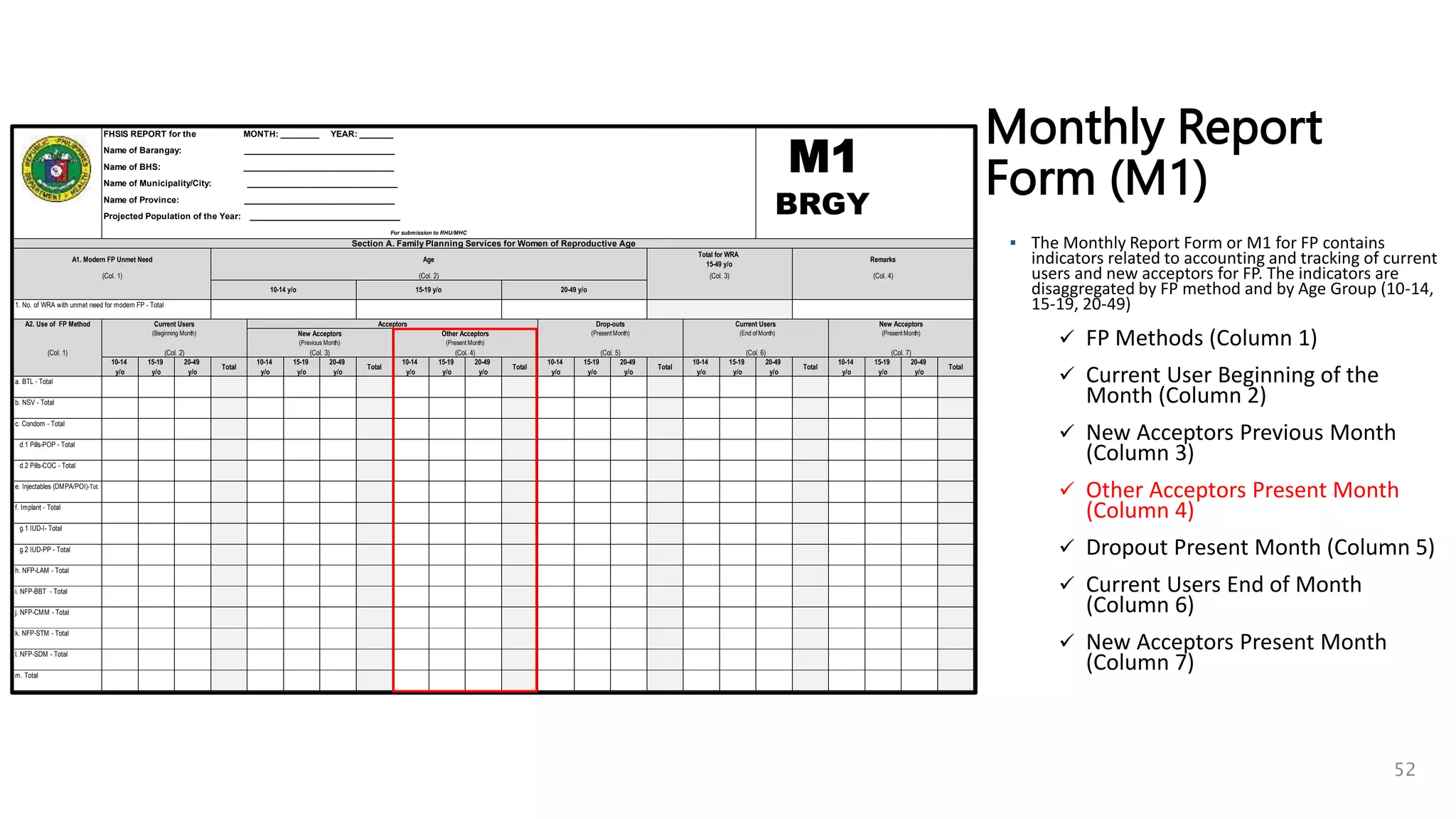
4. Determine the number of Other Acceptors of the Present Month by FP method
and by Age Group (10-14, 15-19, 20-49) [TCL: refer to date of registration
and Type of Client is CC, CM, RS]
56](https://image.slidesharecdn.com/hisfhsisprocessformsdqcprocessandtools-copy-230713071446-f7c63452/75/HIS-FHSIS-process-forms-DQC-process-and-Tools-Copy-pptx-56-2048.jpg)
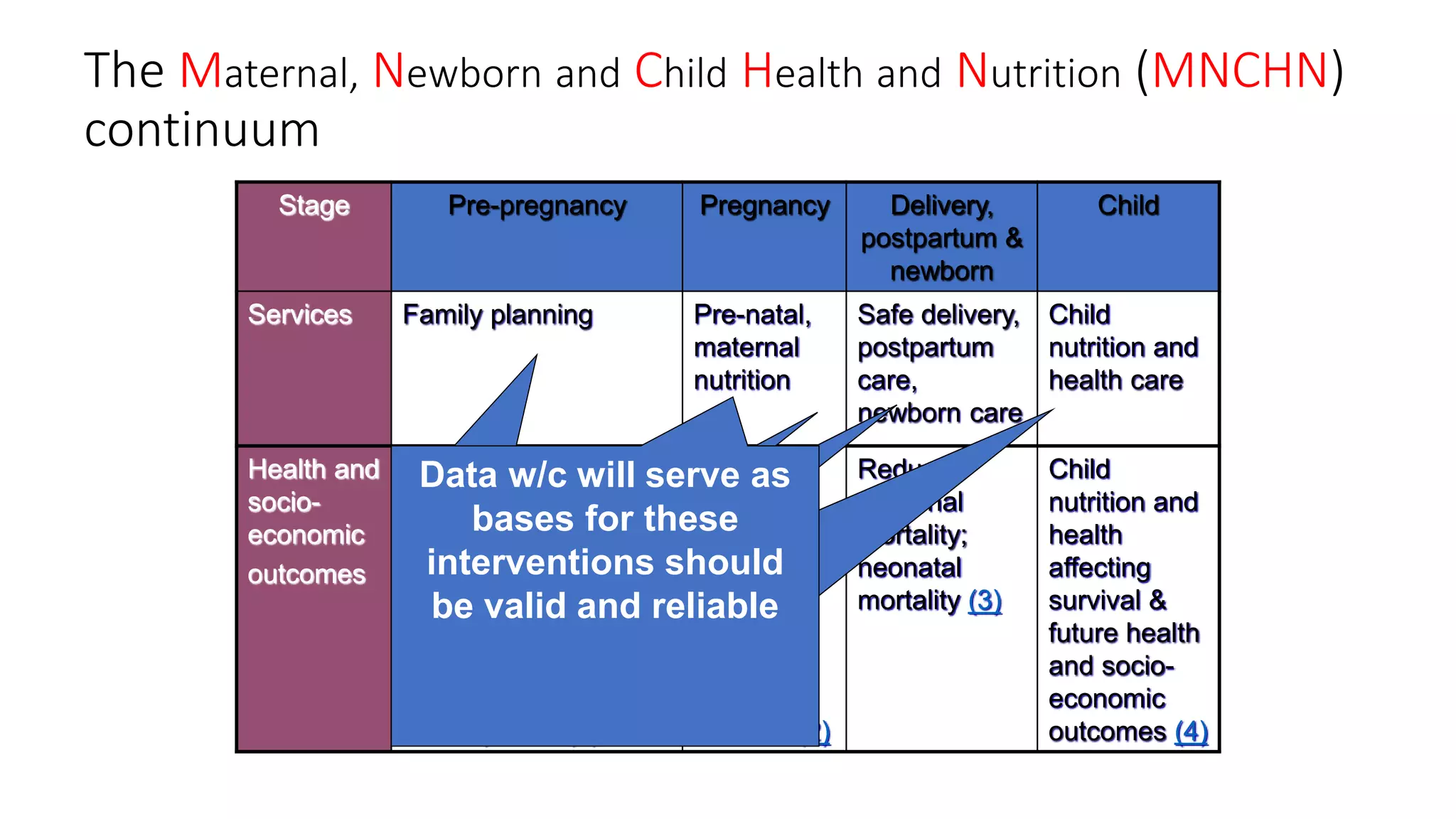
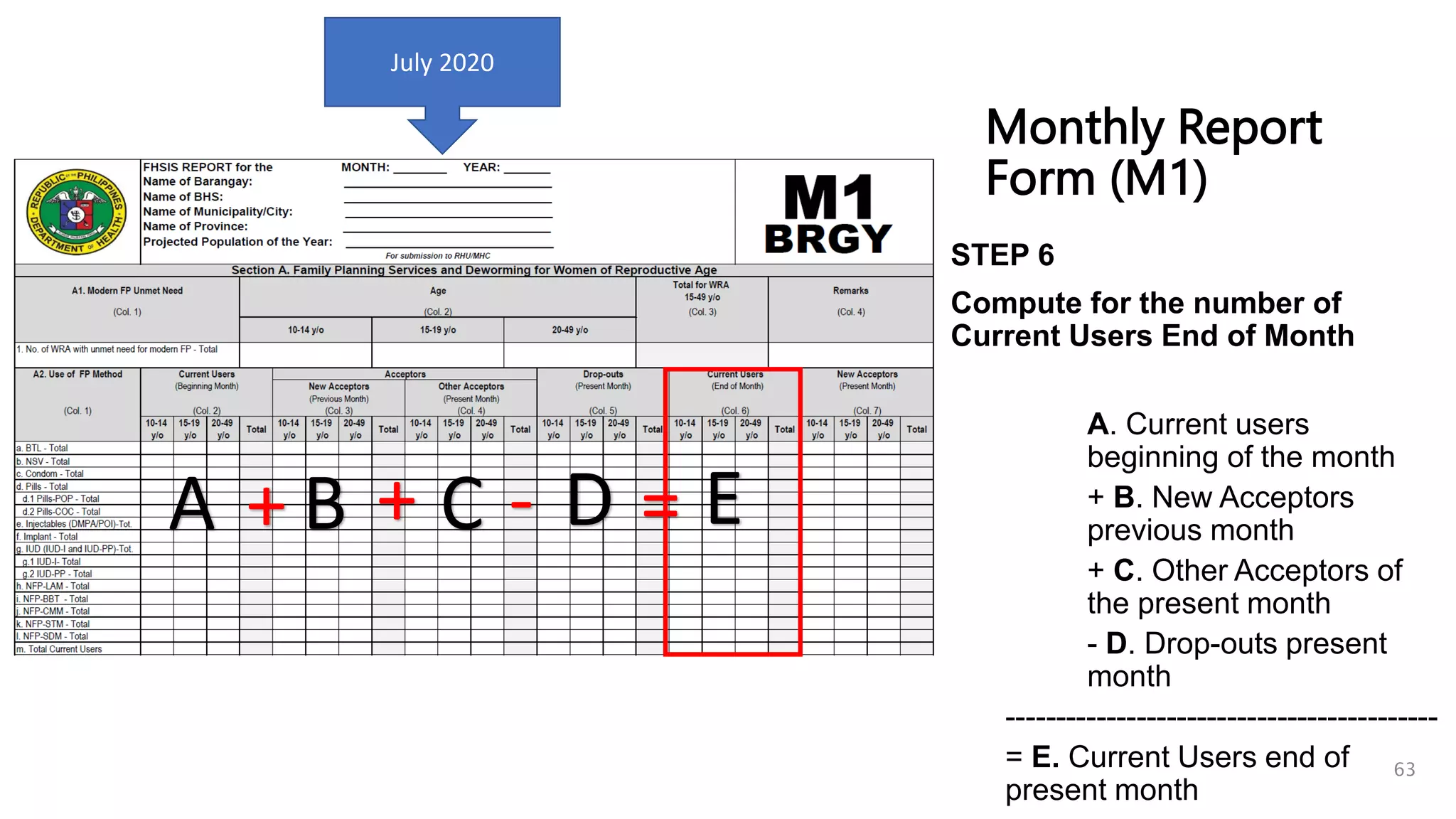
![5. Determine the number of Drop-outs by FP method and by Age Group (10-14, 15-
19, 20-49) [TCL: refer to Dropout date]
6. Compute for Current Users End of Month using the following formula:
Ex. Preparing for M1 of July
Current Users for Beginning of July (Equal to CU End of Month of June)
+ Total New Acceptors of the Previous Month (Equal to NA Present of June)
+ Total Other Acceptors for the Current Month (Equal to OA of July)
- Drop-outs (Count the clients in TCL with July Dropout Date)
57](https://image.slidesharecdn.com/hisfhsisprocessformsdqcprocessandtools-copy-230713071446-f7c63452/75/HIS-FHSIS-process-forms-DQC-process-and-Tools-Copy-pptx-57-2048.jpg)
![10-14
y/o
15-19
y/o
20-49
y/o
Total
10-14
y/o
15-19
y/o
20-49
y/o
Total
10-14
y/o
15-19
y/o
20-49
y/o
Total
10-14
y/o
15-19
y/o
20-49
y/o
Total
10-14
y/o
15-19
y/o
20-49
y/o
Total
10-14
y/o
15-19
y/o
20-49
y/o
Total
a. BTL - Total
b. NSV - Total
c. Condom - Total
d.1 Pills-POP - Total
d.2 Pills-COC - Total
e. Injectables (DMPA/POI)-Tot.
f. Implant - Total
g.1 IUD-I- Total
g.2 IUD-PP - Total
h. NFP-LAM - Total
i. NFP-BBT - Total
j. NFP-CMM - Total
k. NFP-STM - Total
l. NFP-SDM - Total
m. Total
Total for WRA
15-49 y/o
(Col. 2)
Age
10-14 y/o 15-19 y/o 20-49 y/o
(End of Month)
Current Users
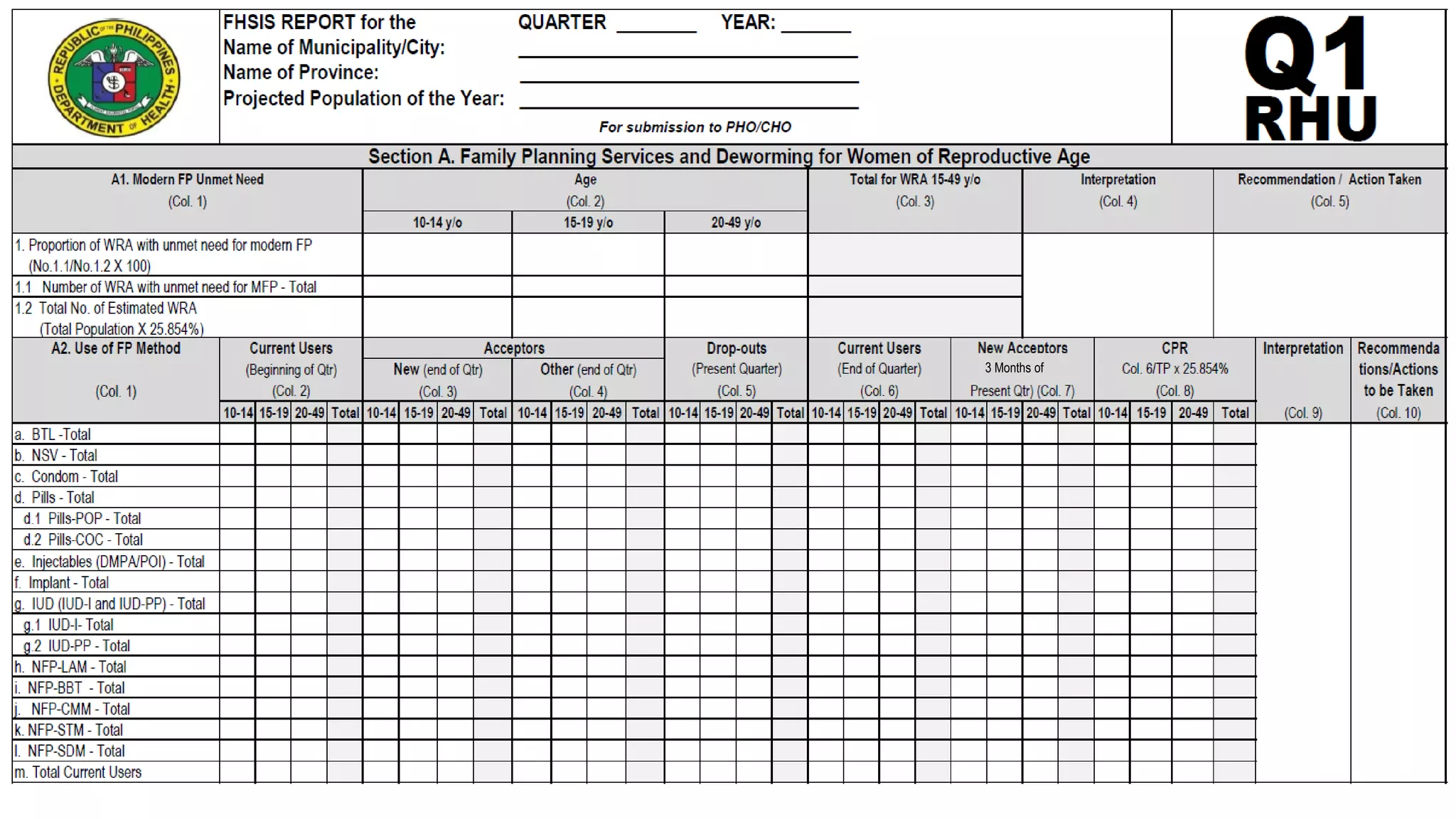
(Col. 1)
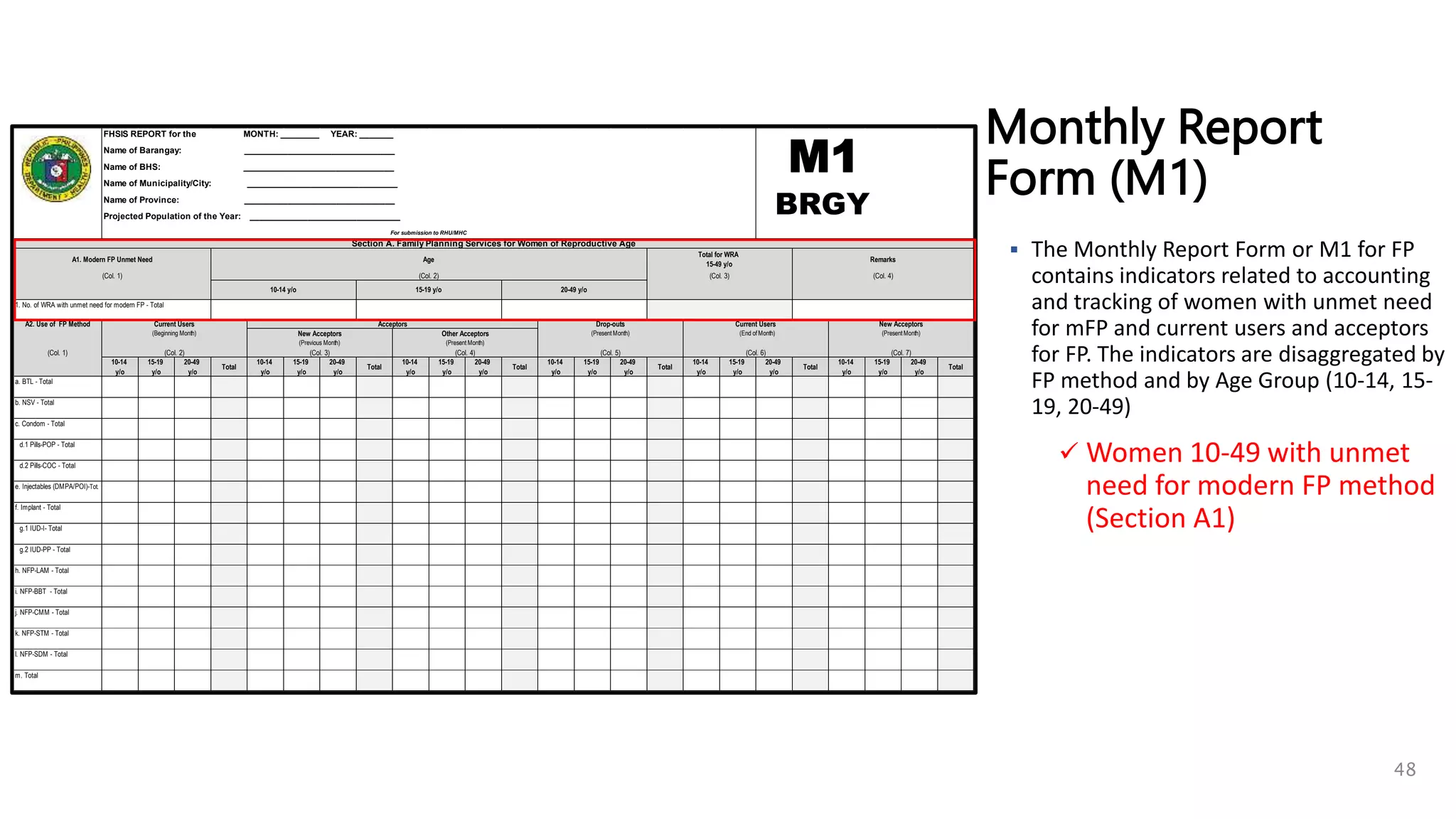
A1. Modern FP Unmet Need
(Col. 4)
Remarks
(Col. 3)
Name of BHS: _______________________________
Name of Barangay: _______________________________
(Present Month)
1. No. of WRA with unmet need for modern FP - Total
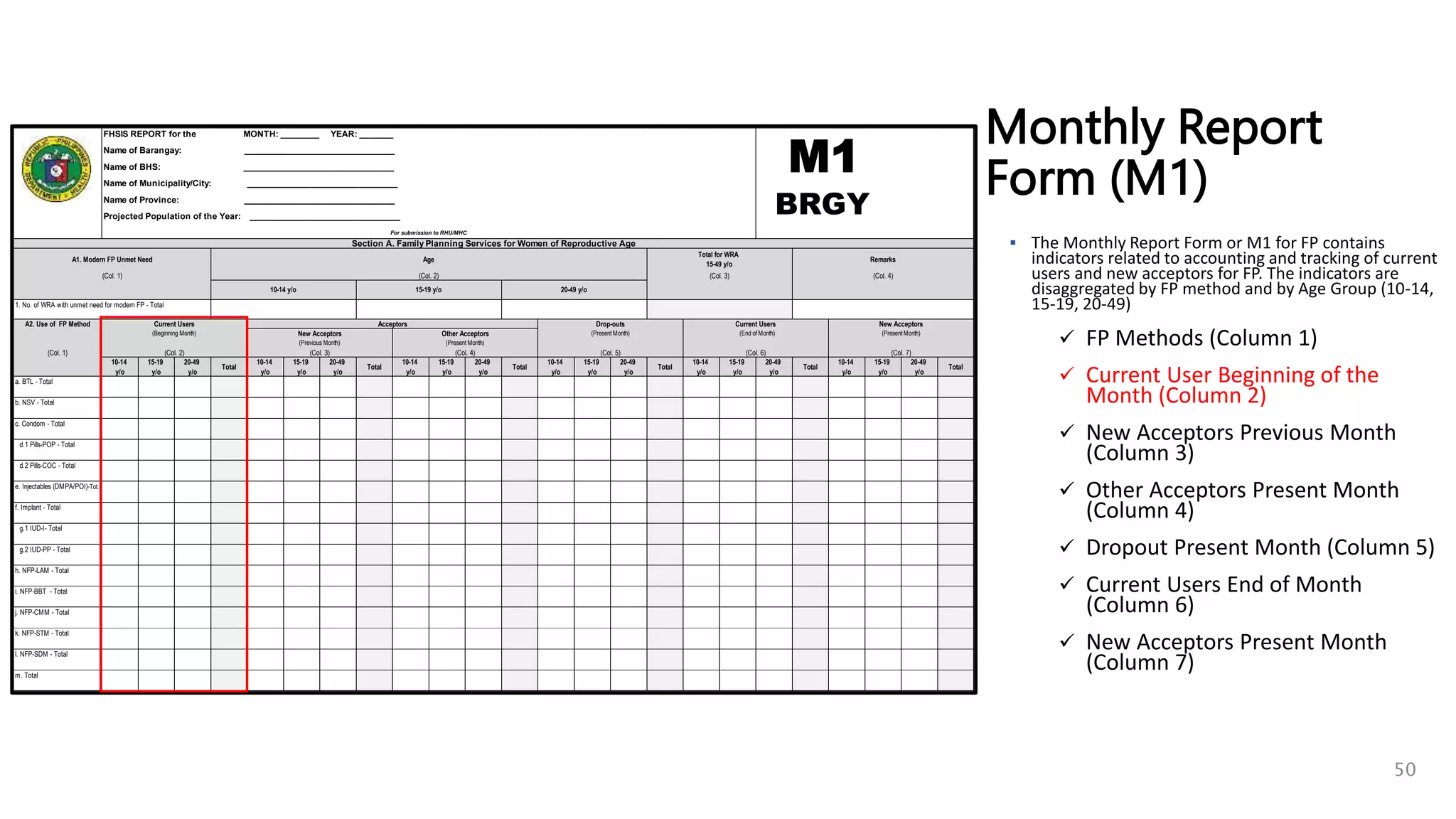
A2. Use of FP Method
(Beginning Month)
Current Users Acceptors
(Col. 5)
(Present Month)
Drop-outs
(Previous Month)
New Acceptors
(Col. 2)
(Col. 1) (Col. 4)
(Present Month)
(Col. 6)
(Col. 3)
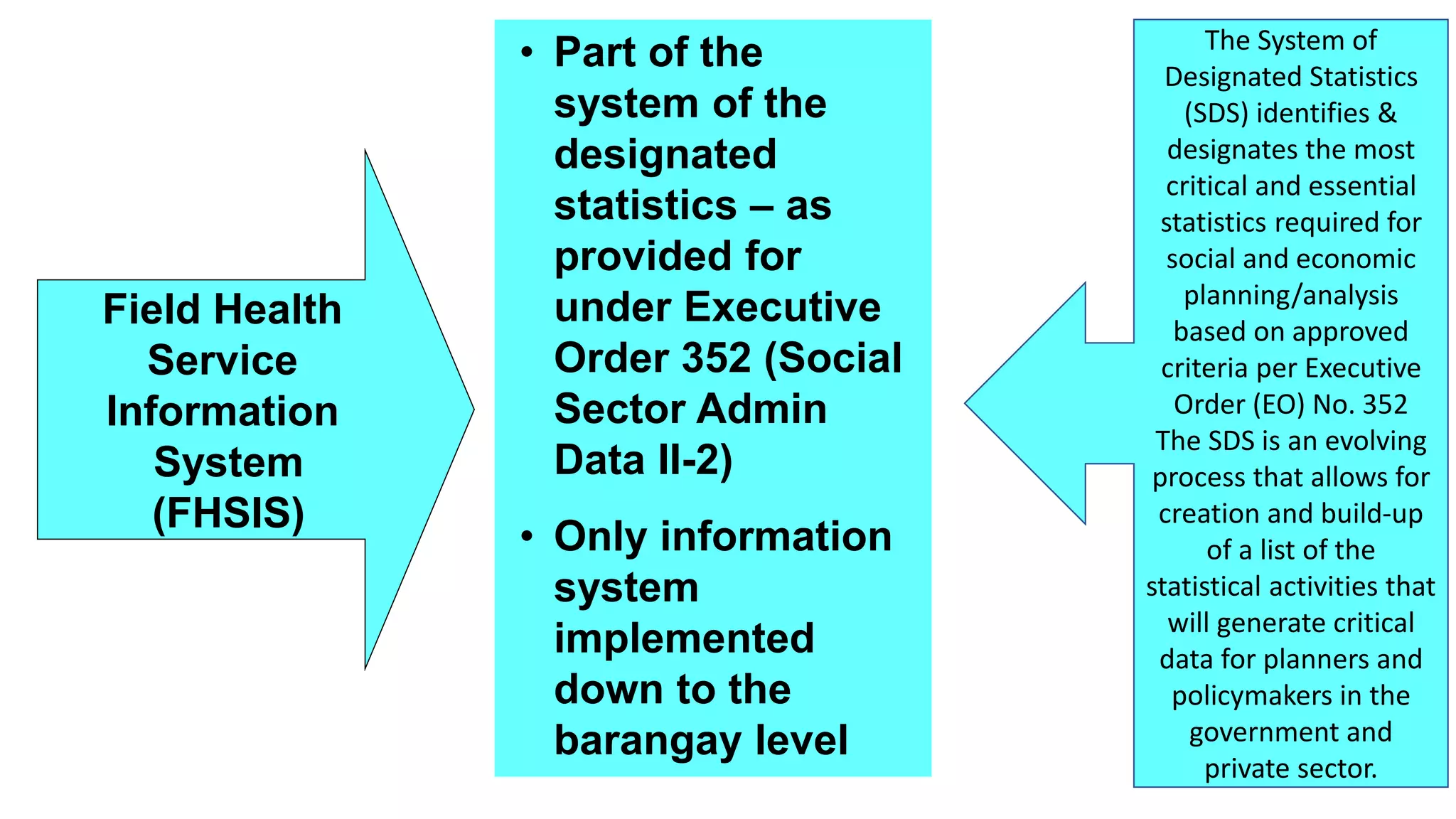
FHSIS REPORT for the MONTH: ________ YEAR: _______
Other Acceptors
Section A. Family Planning Services for Women of Reproductive Age
New Acceptors
(Col. 7)
For submission to RHU/MHC
Projected Population of the Year: _______________________________
Name of Province: _______________________________
Name of Municipality/City: _______________________________
BRGY
Monthly Report
Form (M1)
STEP 1
Determine the Current
Users Beginning of Month
by FP method and by Age
Group (10-14, 15-19, 20-49)
[This is equivalent to
Current Users End of
Previous Month] or copy
Column 6 from M1 of
Previous Month
58
June 2020
July 2020](https://image.slidesharecdn.com/hisfhsisprocessformsdqcprocessandtools-copy-230713071446-f7c63452/75/HIS-FHSIS-process-forms-DQC-process-and-Tools-Copy-pptx-58-2048.jpg)

![Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Date Reason****
6
7
8
9
10
1
2
3
4
5
________________________ (Name of FP Method)
FOLLOW-UP VISITS
(Upper Space: Schedule Date of next visit / Lower Space: Actual Date of Visit)
(10)
DROP-OUT
(11)
Remarks/
Actions Taken
(12)
No.
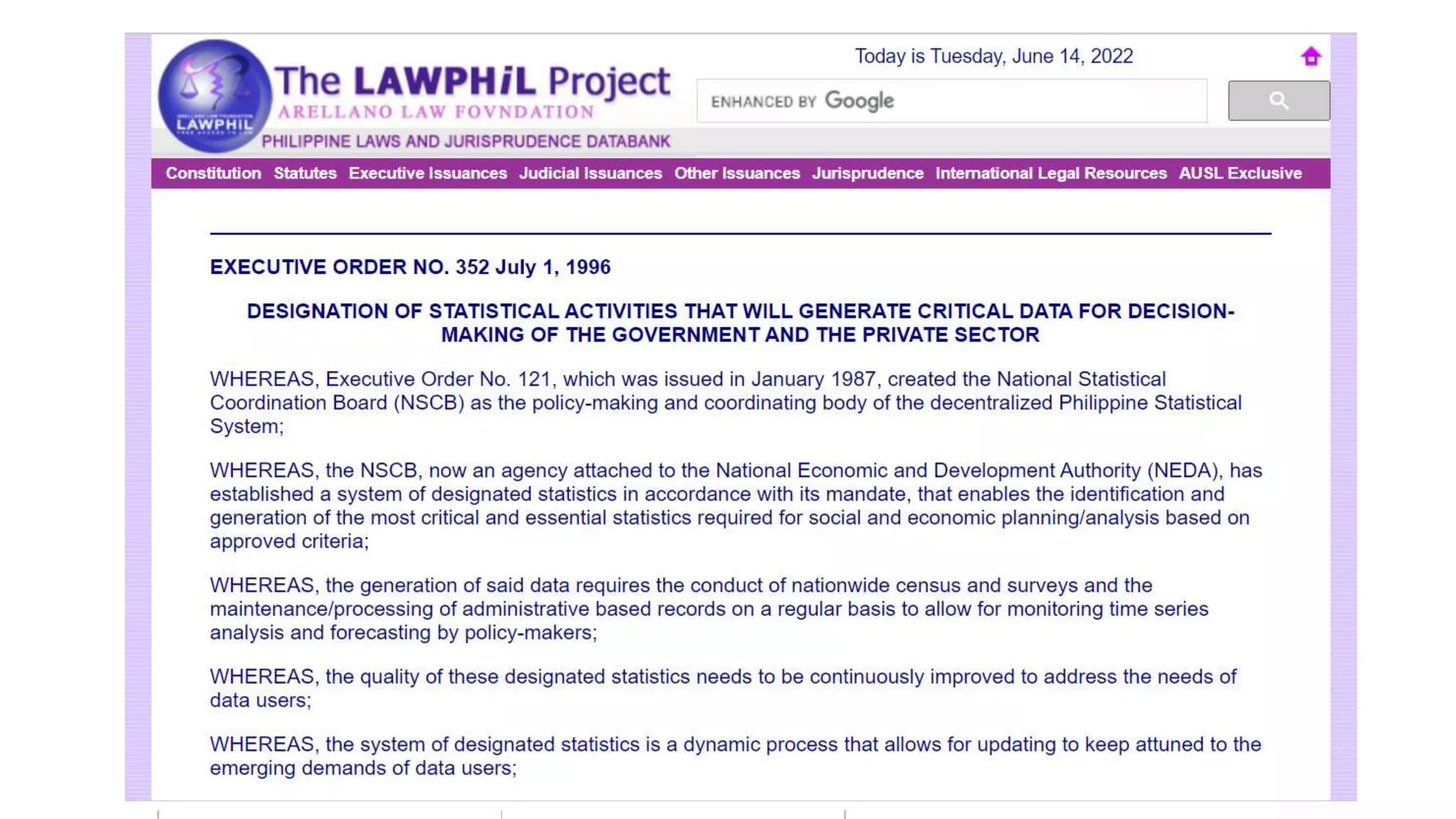
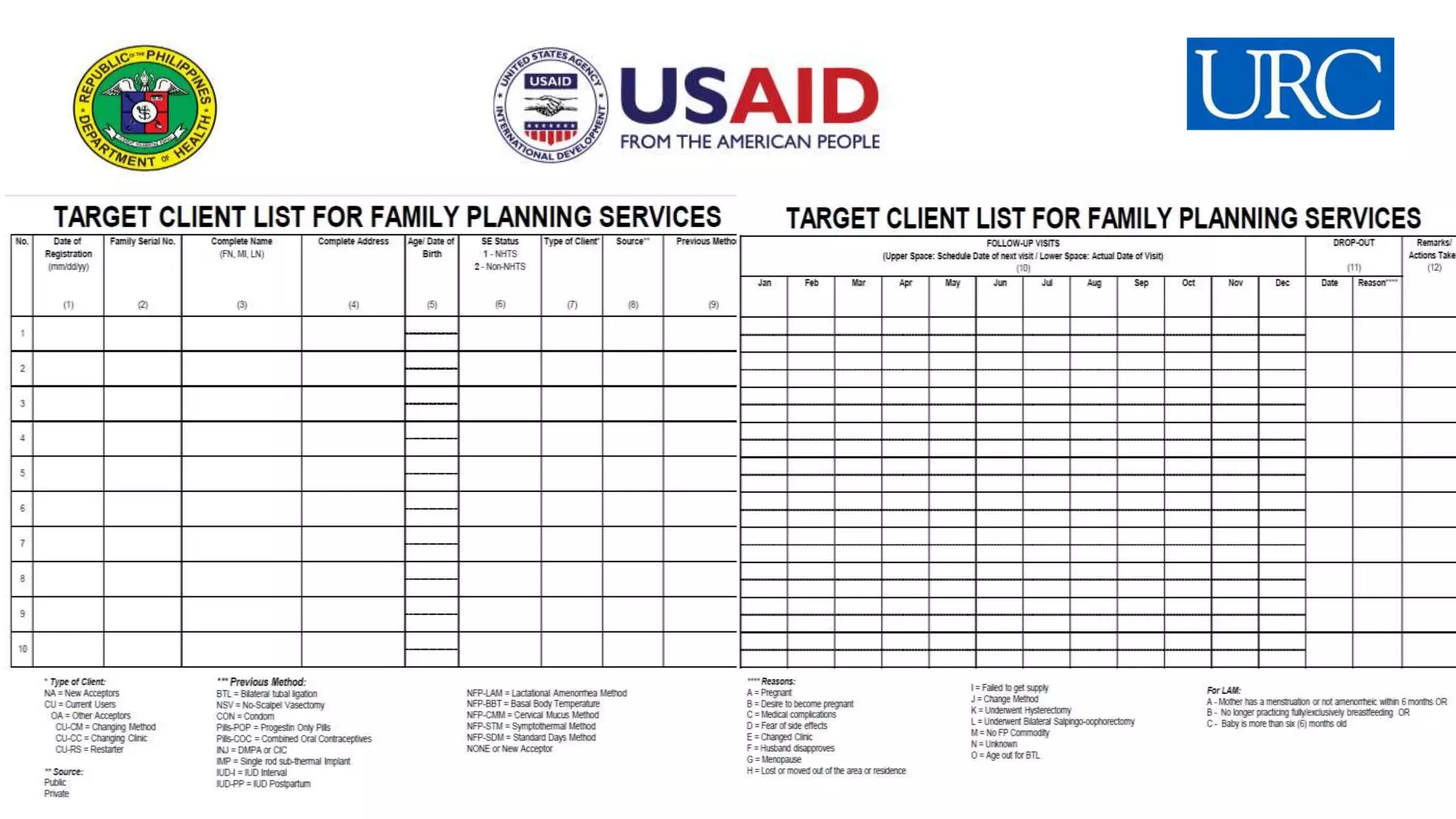
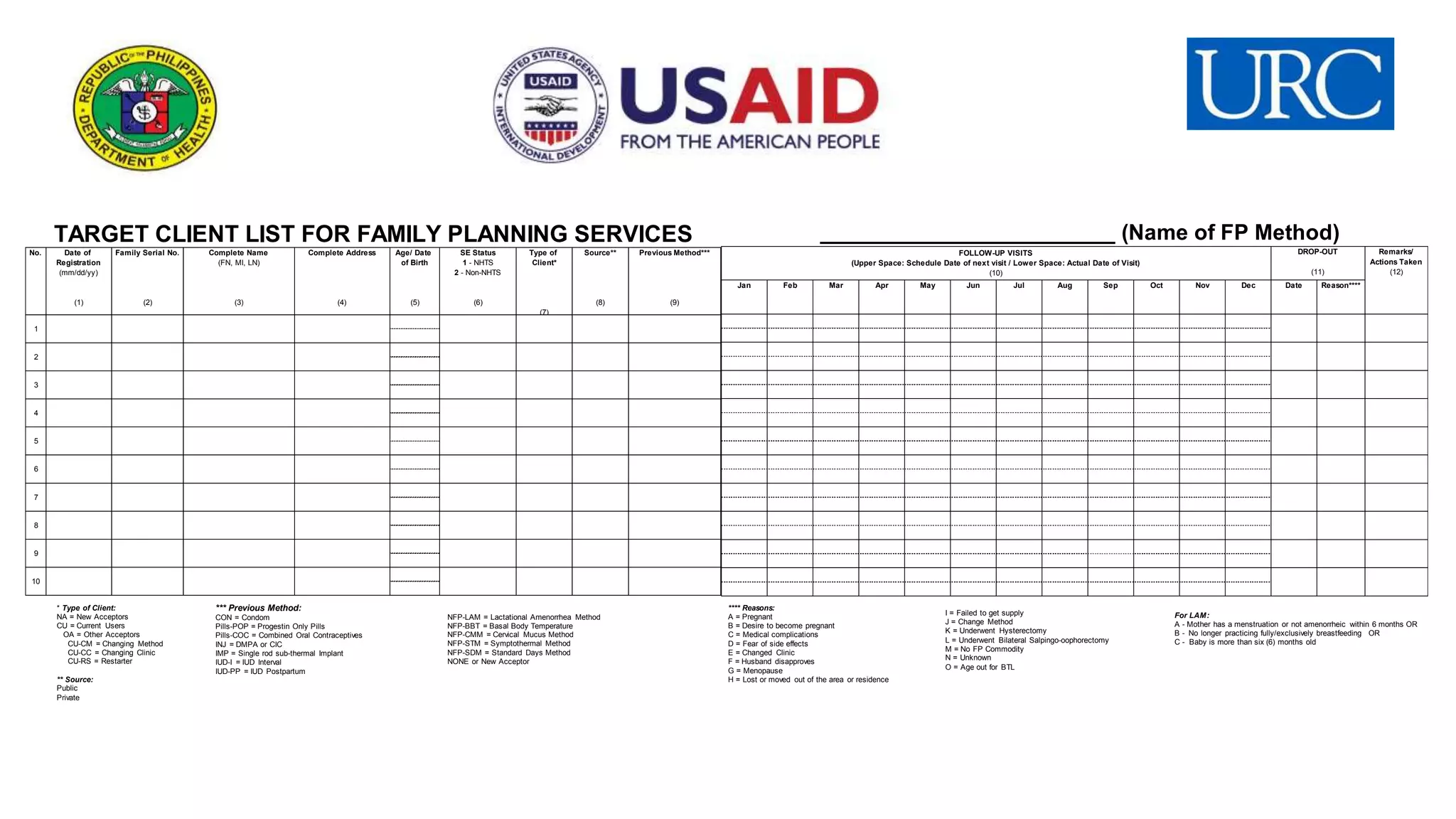
TARGET CLIENT LIST FOR FAMILY PLANNING SERVICES
Previous Method***
(9)
Complete Address
(4)
Complete Name
(FN, MI, LN)
(3)
Family Serial No.
(2)
Date of
Registration
(mm/dd/yy)
(1)
Type of
Client*
(7)
SE Status
1 - NHTS
2 - Non-NHTS
(6)
Age/ Date
of Birth
(5)
Source**
(8)
* Type of Client:
NA = New Acceptors
CU = Current Users
OA = Other Acceptors
CU-CM = Changing Method
CU-CC = Changing Clinic
CU-RS = Restarter
** Source:
Public
Private
*** Previous Method:
CON = Condom
Pills-POP = Progestin Only Pills
Pills-COC = Combined Oral Contraceptives
INJ = DMPA or CIC
IMP = Single rod sub-thermal Implant
IUD-I = IUD Interval
IUD-PP = IUD Postpartum
NFP-LAM = Lactational Amenorrhea Method
NFP-BBT = Basal Body Temperature
NFP-CMM = Cervical Mucus Method
NFP-STM = Symptothermal Method
NFP-SDM = Standard Days Method
NONE or New Acceptor
**** Reasons:
A = Pregnant
B = Desire to become pregnant
C = Medical complications
D = Fear of side effects
E = Changed Clinic
F = Husband disapproves
G = Menopause
H = Lost or moved out of the area or residence
I = Failed to get supply
J = Change Method
K = Underwent Hysterectomy
L = Underwent Bilateral Salpingo-oophorectomy
M = No FP Commodity
N = Unknown
O = Age out for BTL
For LAM:
A - Mother has a menstruation or not amenorrheic within 6 months OR
B - No longer practicing fully/exclusively breastfeeding OR
C - Baby is more than six (6) months old
Monthly Report
Form (M1)
STEP 3
Determine the number New
Acceptors of the Present
Month by FP method and by
Age Group (10-14, 15-19, 20-49)
[TCL: refer to date of
registration and Type of Client
is NA] 60
July 2020](https://image.slidesharecdn.com/hisfhsisprocessformsdqcprocessandtools-copy-230713071446-f7c63452/75/HIS-FHSIS-process-forms-DQC-process-and-Tools-Copy-pptx-60-2048.jpg)
![Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Date Reason****
6
7
8
9
10
1
2
3
4
5
________________________ (Name of FP Method)
FOLLOW-UP VISITS
(Upper Space: Schedule Date of next visit / Lower Space: Actual Date of Visit)
(10)
DROP-OUT
(11)
Remarks/
Actions Taken
(12)
No.
TARGET CLIENT LIST FOR FAMILY PLANNING SERVICES
Previous Method***
(9)
Complete Address
(4)
Complete Name
(FN, MI, LN)
(3)
Family Serial No.
(2)
Date of
Registration
(mm/dd/yy)
(1)
Type of
Client*
(7)
SE Status
1 - NHTS
2 - Non-NHTS
(6)
Age/ Date
of Birth
(5)
Source**
(8)
* Type of Client:
NA = New Acceptors
CU = Current Users
OA = Other Acceptors
CU-CM = Changing Method
CU-CC = Changing Clinic
CU-RS = Restarter
** Source:
Public
Private
*** Previous Method:
CON = Condom
Pills-POP = Progestin Only Pills
Pills-COC = Combined Oral Contraceptives
INJ = DMPA or CIC
IMP = Single rod sub-thermal Implant
IUD-I = IUD Interval
IUD-PP = IUD Postpartum
NFP-LAM = Lactational Amenorrhea Method
NFP-BBT = Basal Body Temperature
NFP-CMM = Cervical Mucus Method
NFP-STM = Symptothermal Method
NFP-SDM = Standard Days Method
NONE or New Acceptor
**** Reasons:
A = Pregnant
B = Desire to become pregnant
C = Medical complications
D = Fear of side effects
E = Changed Clinic
F = Husband disapproves
G = Menopause
H = Lost or moved out of the area or residence
I = Failed to get supply
J = Change Method
K = Underwent Hysterectomy
L = Underwent Bilateral Salpingo-oophorectomy
M = No FP Commodity
N = Unknown
O = Age out for BTL
For LAM:
A - Mother has a menstruation or not amenorrheic within 6 months OR
B - No longer practicing fully/exclusively breastfeeding OR
C - Baby is more than six (6) months old
Monthly Report
Form (M1)
STEP 4
Determine the number Other
Acceptors of the Present Month
by FP method and by Age Group
(10-14, 15-19, 20-49)
[TCL: refer to date of
registration and Type of Client
is CM, CC, or RS] 61
July 2020](https://image.slidesharecdn.com/hisfhsisprocessformsdqcprocessandtools-copy-230713071446-f7c63452/75/HIS-FHSIS-process-forms-DQC-process-and-Tools-Copy-pptx-61-2048.jpg)
![Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Date Reason****
6
7
8
9
10
1
2
3
4
5
________________________ (Name of FP Method)
FOLLOW-UP VISITS
(Upper Space: Schedule Date of next visit / Lower Space: Actual Date of Visit)
(10)
DROP-OUT
(11)
Remarks/
Actions Taken
(12)
No.
TARGET CLIENT LIST FOR FAMILY PLANNING SERVICES
Previous Method***
(9)
Complete Address
(4)
Complete Name
(FN, MI, LN)
(3)
Family Serial No.
(2)
Date of
Registration
(mm/dd/yy)
(1)
Type of
Client*
(7)
SE Status
1 - NHTS
2 - Non-NHTS
(6)
Age/ Date
of Birth
(5)
Source**
(8)
* Type of Client:
NA = New Acceptors
CU = Current Users
OA = Other Acceptors
CU-CM = Changing Method
CU-CC = Changing Clinic
CU-RS = Restarter
** Source:
Public
Private
*** Previous Method:
CON = Condom
Pills-POP = Progestin Only Pills
Pills-COC = Combined Oral Contraceptives
INJ = DMPA or CIC
IMP = Single rod sub-thermal Implant
IUD-I = IUD Interval
IUD-PP = IUD Postpartum
NFP-LAM = Lactational Amenorrhea Method
NFP-BBT = Basal Body Temperature
NFP-CMM = Cervical Mucus Method
NFP-STM = Symptothermal Method
NFP-SDM = Standard Days Method
NONE or New Acceptor
**** Reasons:
A = Pregnant
B = Desire to become pregnant
C = Medical complications
D = Fear of side effects
E = Changed Clinic
F = Husband disapproves
G = Menopause
H = Lost or moved out of the area or residence
I = Failed to get supply
J = Change Method
K = Underwent Hysterectomy
L = Underwent Bilateral Salpingo-oophorectomy
M = No FP Commodity
N = Unknown
O = Age out for BTL
For LAM:
A - Mother has a menstruation or not amenorrheic within 6 months OR
B - No longer practicing fully/exclusively breastfeeding OR
C - Baby is more than six (6) months old
Monthly Report
Form (M1)
STEP 5
Determine the number of Drop-
outs by FP method and by Age
Group (10-14, 15-19, 20-49)
[TCL: refer to Dropout date and
count the clients with dropout
dates; Make sure the TCL is
updated] 62
July 2020](https://image.slidesharecdn.com/hisfhsisprocessformsdqcprocessandtools-copy-230713071446-f7c63452/75/HIS-FHSIS-process-forms-DQC-process-and-Tools-Copy-pptx-62-2048.jpg)










![MAJOR INDICATORS FOR FP PROGRAM
IMPLEMENTATION:
WOMEN ABLE TO ACCESS
FP METHODS OF THEIR CHOICE
[NO. OF FPCU; CONTRACEPTIVE PREVALENCE RATE (CPR)]
COMMODITY SECURITY (REDUCTION/ELIMINATION OF FP
COMMODITY STOCK-OUTS)
INCREASED CAPACITIES FOR FP SERVICE PROVISION
INCREASED DEMAND FOR FP SERVICES
REDUCTION/ELIMINATION OF
UNMET NEEDS FOR FP](https://image.slidesharecdn.com/hisfhsisprocessformsdqcprocessandtools-copy-230713071446-f7c63452/75/HIS-FHSIS-process-forms-DQC-process-and-Tools-Copy-pptx-89-2048.jpg)

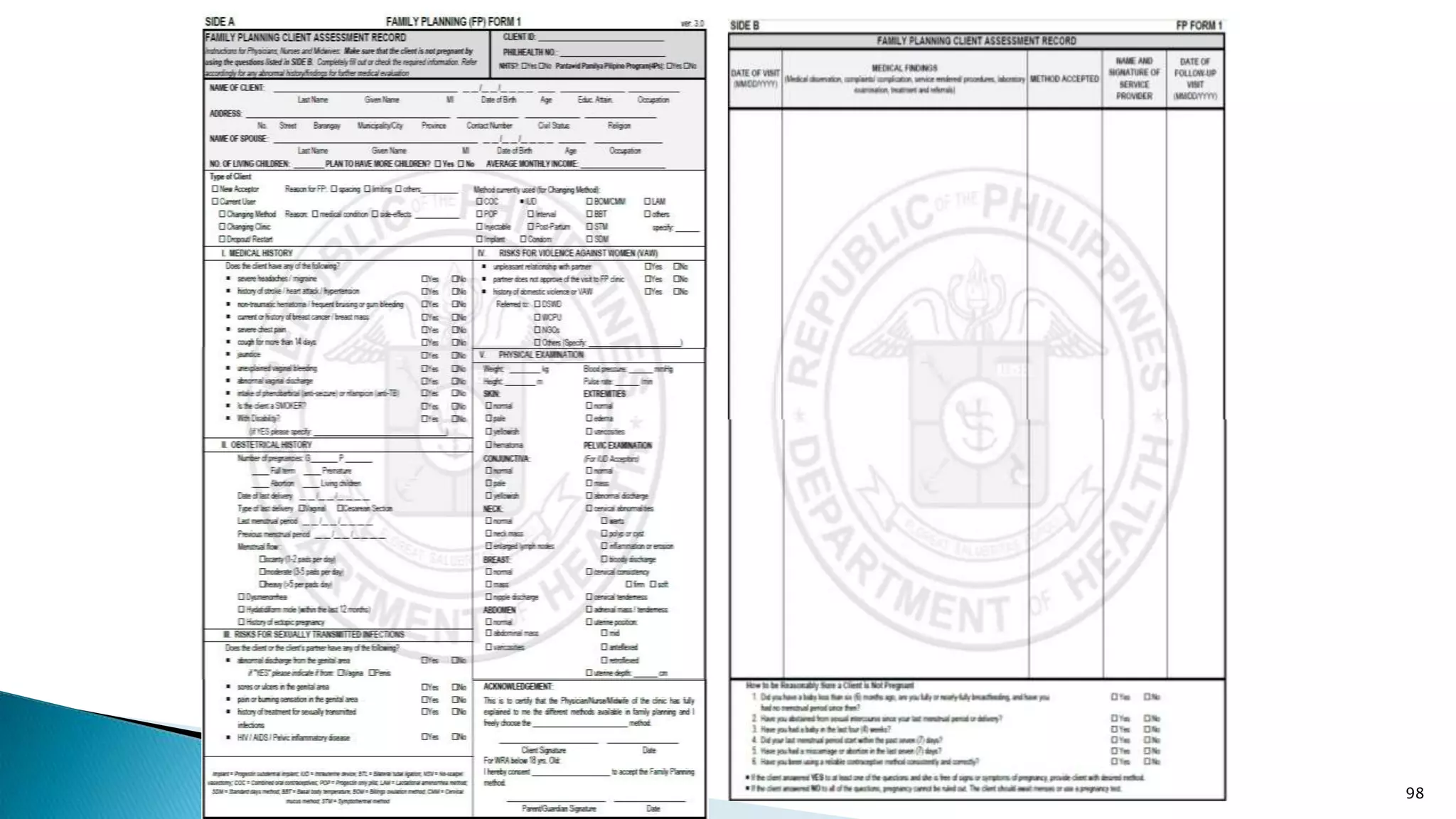
![IV. RECORDING FORMS
1. LIST OF POTENTIAL CLIENTS
96
Sex
(M or F)
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
TOTAL
LIST OF POTENTIAL FP CLIENTS
Contact Number
Remarks
[Can include information
on w here the patient w as
initially seen/identified
(e.g. Ward, OPD, Pedia)]
Year: __________ Month ____________
Date Name of Potential FP Client Age
Gravida/
Para
(G/P)
Address
All clients with potential unmet needs for FP
shall be recorded in the LIST OF POTENTIAL
CLIENTS; will include:
• clients who expressed intention to
use an FP method but have not yet
been provided with either information
or services
• clients who have been provided with
initial information through group
information-giving but have not yet
been provided with actual FP services.](https://image.slidesharecdn.com/hisfhsisprocessformsdqcprocessandtools-copy-230713071446-f7c63452/75/HIS-FHSIS-process-forms-DQC-process-and-Tools-Copy-pptx-95-2048.jpg)
















![V. REPORTING FORMS
1. Monthly Form (M1)
STEPS IN PREPARING FOR THE MONTHLY FORM (M1):
1. Determine the Current Users for Beginning of April (2016)
[This is equivalent to Current Users as of previous month: March
2016]
2. Add the Total New Acceptors of the previous Month (March
2016)
3. Add the Total Other Acceptors (April 2016)
4. Deduct the Drop-outs for the Current Month (April 2016)
Example:
FPCU (as of end of April 2016) =
Current Users for Beginning of April (Equal to End of Month of
March) = 189
+ Total New Acceptors of the Previous Month = 33
+ Total Other Acceptors for the Current Month = 13
- Drop-outs = 5
Thus FPCU end of April 2016 = 230 115](https://image.slidesharecdn.com/hisfhsisprocessformsdqcprocessandtools-copy-230713071446-f7c63452/75/HIS-FHSIS-process-forms-DQC-process-and-Tools-Copy-pptx-114-2048.jpg)