Downloaded 950 times


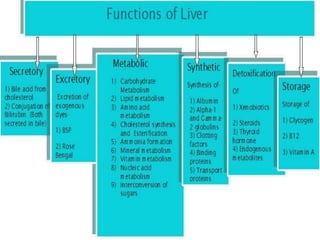

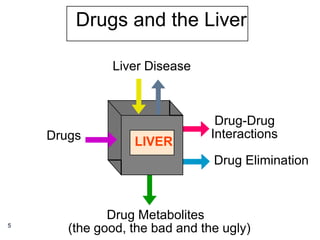



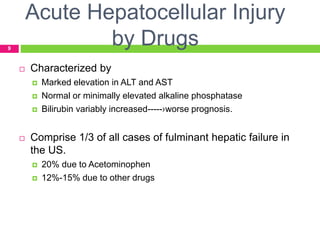
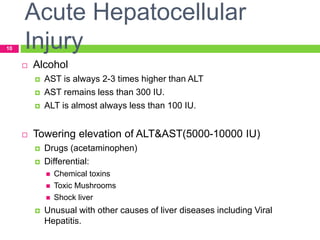





























































1) The liver plays a key role in metabolism and detoxification, and is susceptible to damage from toxins like alcohol, chemicals, and certain drugs. 2) Drugs are a common cause of liver injury (DILI), with anti-tuberculosis drugs, anti-convulsants, NSAIDs, anti-microbials, and anesthetics carrying risks. DILI can range from asymptomatic enzyme elevations to acute liver failure. 3) Many agents have hepatoprotective properties, including N-acetylcysteine, penicillamine, antioxidants, S-adenosylmethionine (SAMe), and herbal medicines like Silybum marianum (































































![Human Reproduction [ Reproductive System ] Notes @irfanullah_mehar Irfanullah...](https://cdn.slidesharecdn.com/ss_thumbnails/humanreproductionreproductivesystemnotesirfanullahmeharirfanullahmeharjanantantra-260111172350-56e85778-thumbnail.jpg?width=640&height=640&fit=bounds)









