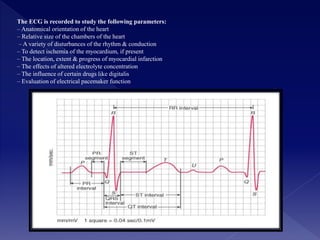
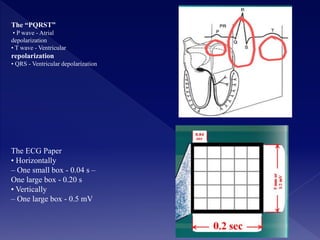
The document discusses the electrocardiograph, which records the electrical activity of the heart in a graphic form called an electrocardiogram (ECG). An ECG can check the heart's rhythm, rate, axis, and state of the myocardial muscle. It has medical applications such as detecting cardiovascular issues. A normal ECG shows the P wave from atrial depolarization, the QRS complex from ventricular depolarization, and the T wave from ventricular repolarization. Abnormalities like tachycardia, bradycardia, and heart block can also be identified on an ECG.




































![Shadechapter01.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter01-150421101218-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)



![ECG [electrocardiogram].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ecgelectrocardiogram-220416062706-thumbnail.jpg?width=640&height=640&fit=bounds)