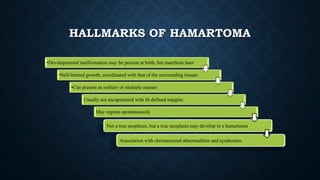
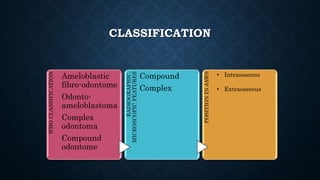
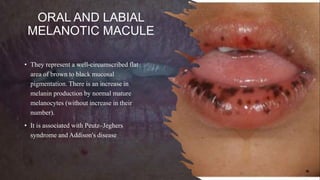
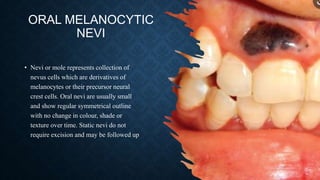
Hamartomas are non-neoplastic developmental malformations that contain a mixture of normally differentiated tissues native to the anatomic site. They can be classified based on their cellular origin, including odontogenic, epithelial, mesenchymal, and syndromic types. Odontogenic hamartomas include dens invaginatus and dens evaginatus, which are developmental anomalies of teeth. Epithelial hamartomas involve tissues like oral melanotic macules. Mesenchymal hamartomas comprise tissues such as blood vessels, muscles, nerves, and bone. Syndromic hamartomas are associated with conditions like Cowden and tuberous sclerosis. Some lesions remain controversial as to whether they represent true hamart