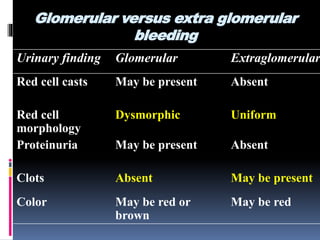
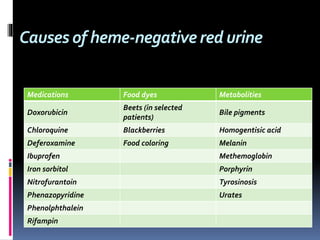
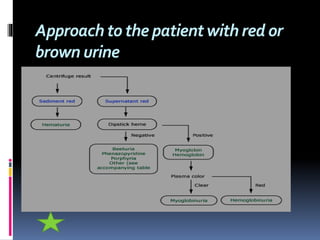
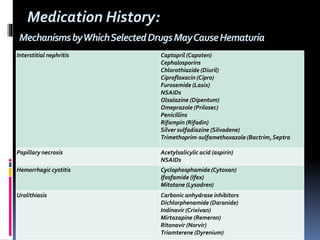
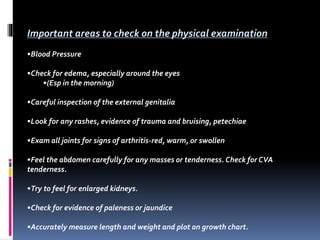
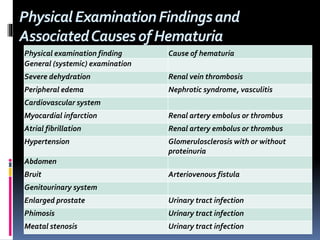
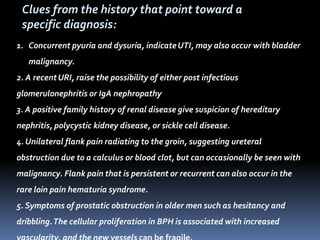
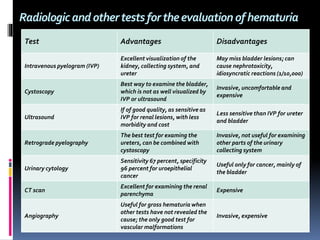
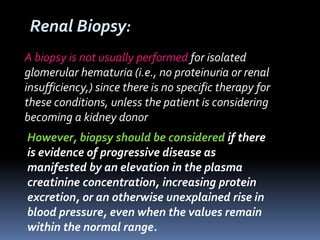
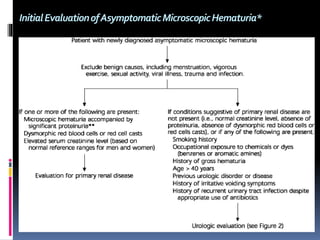
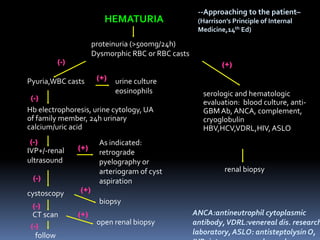
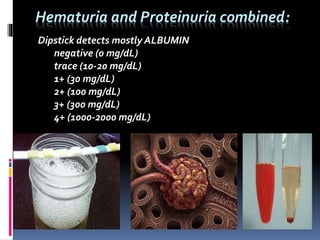
The document discusses the evaluation of hematuria. It defines macroscopic and microscopic hematuria and provides a classification. Important clues from the history and physical exam are outlined that can point to specific diagnoses. Distinguishing between glomerular and extraglomerular bleeding is important. Common causes of hematuria are reviewed including those related to the kidney, urinary tract, and unrelated conditions. Transient versus persistent hematuria is an important distinction to make in guiding evaluation and workup. Recommended initial laboratory tests and potential radiologic tests are presented.