Downloaded 139 times
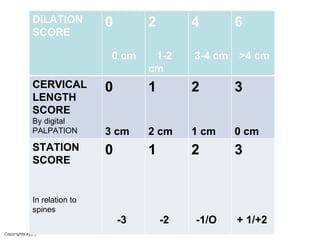
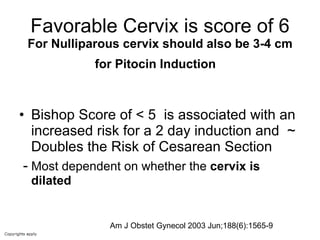
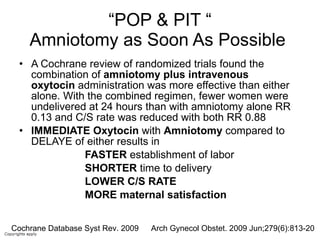

The document provides guidelines for cervical ripening and labor induction. Key points include: - The modified Bishop score is the best tool for predicting successful induction outcomes. Cervical dilation carries the most weight. - Early amniotomy and oxytocin ("pop and pit") results in faster labor onset, shorter delivery time, and lower C-section rates compared to delayed amniotomy or oxytocin alone. - Outpatient cervical ripening with misoprostol (Cytotec) should allow assessment for admission or discharge by 8:30am following the induction attempt.























































































