Downloaded 918 times
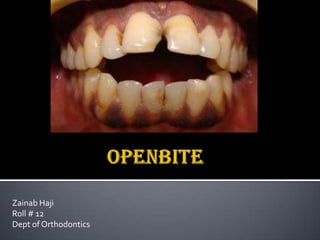
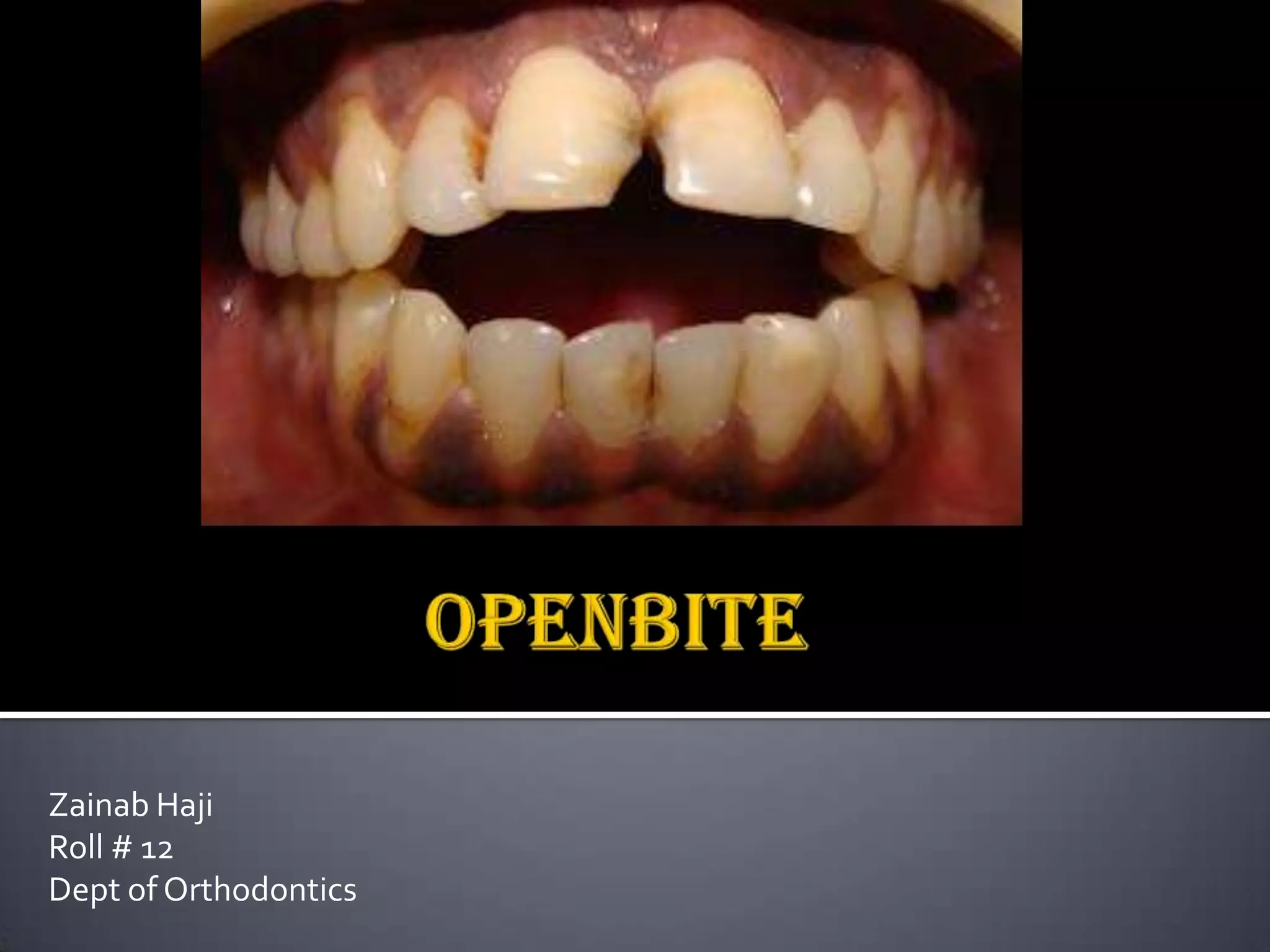
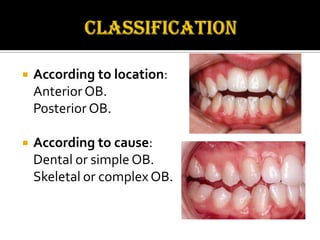

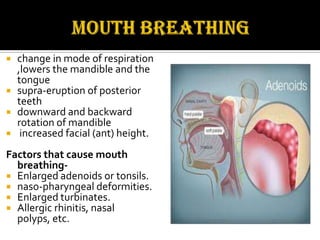
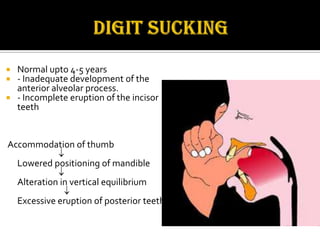
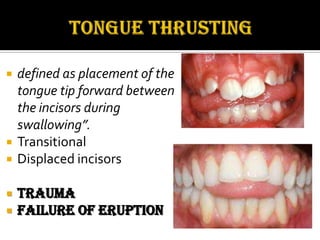

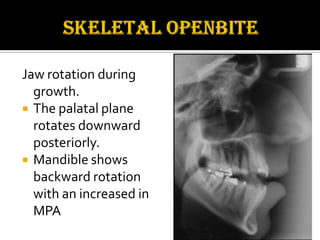
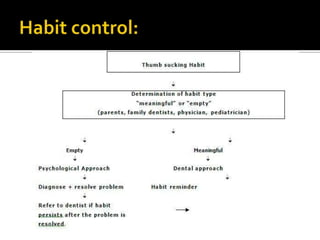
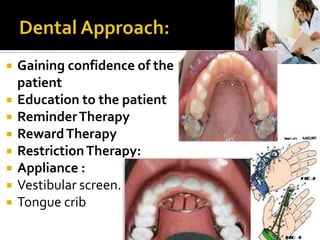
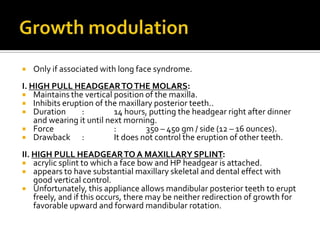
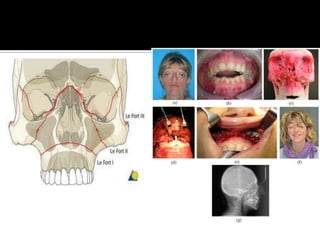

This document discusses open bite, including its definition, classification, causes, and management. Open bite is classified as anterior, posterior, dental/simple, or skeletal/complex. Causes include hereditary factors, environmental factors like mouth breathing, thumb sucking, and trauma. Management depends on the patient's age and involves things like habit control, growth modulation, functional appliances with bite blocks, and sometimes orthognathic surgery. High pull headgear is discussed as a way to control vertical growth.



















































































