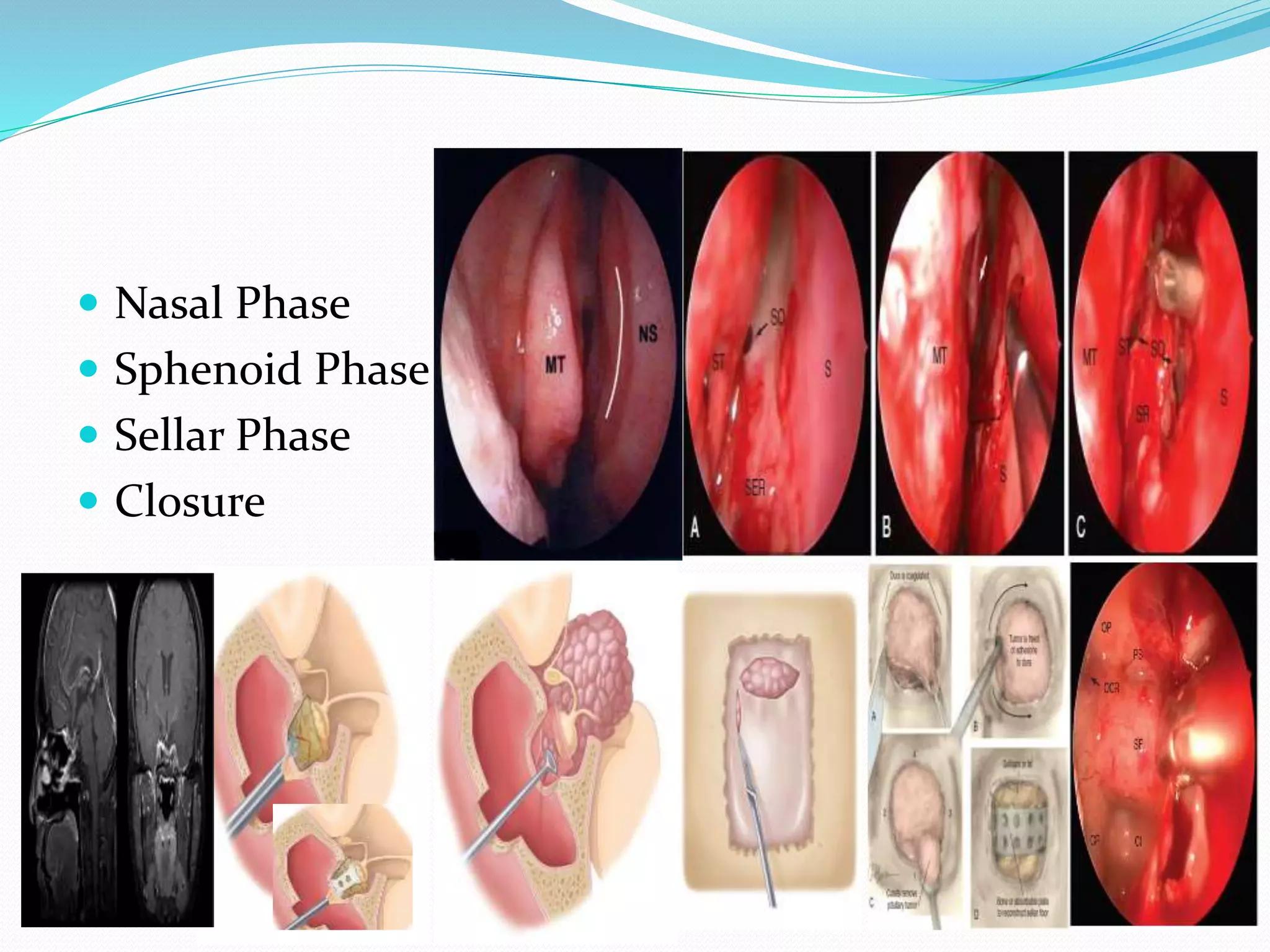
This document discusses acromegaly, a rare disorder caused by excess growth hormone secretion from the pituitary gland after epiphyseal closure. It presents in adults with coarse facial features, joint pain, and organ enlargement. Diagnosis involves blood tests and imaging of the pituitary. Treatment options include surgery, radiation, or medication to reduce growth hormone levels. The trans-sphenoidal surgical approach is described which involves accessing the pituitary through the nasal cavity and sphenoid sinus. Risks of surgery include bleeding, infection, and damage to nearby structures.