1) Smile esthetics is influenced by factors like gingival tissue display, contour, and position of interdental papillae. Gingival esthetics play an important role in orthodontic treatment.
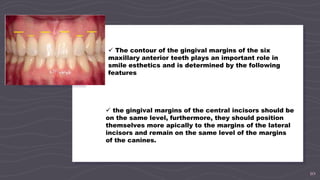
2) Gingival contour is divided into microesthetics (dental aspects), miniesthetics (smile dynamics), and macroesthetics (facial harmony). Ideal gingival contours follow bone architecture and have parallel gingival margins and coinciding contour/clinical crown emergence.
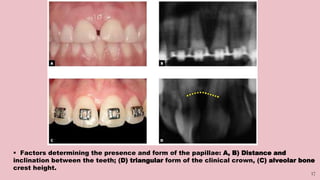
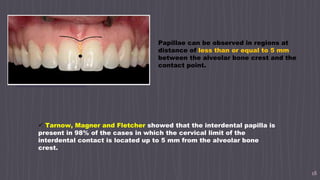
3) Interdental papillae presence is influenced by distance between contact point and bone crest. Papillae are generally present when this distance is ≤5mm and absent when >7mm,