Downloaded 99 times




![Variety of lip:
a. According to functional capacity:
i. Competent lip
ii. Incompetent lip
iii. Strap like lower lip
iv. Everted lip
b. According to tonicity [Feel the lip for consistency]:
i. Normal: Minimum consistency present.
ii. Hypertonic: Tends to be firm & redder
iii. Hypotonic: Lip is flaccid
c. According to expressive behavior:
i. Normal
ii. Over active
iii. Under active.
LIPS](https://image.slidesharecdn.com/softtissuemorphology-180622062945/85/Soft-tissue-morphology-6-320.jpg)







![• The cheek has moulding
effect on the buccal or
posterior teeth. [Lip has
moulding effect on
anterior teeth]
• These effect of cheek
(and lip) are counteracted
by the tongue.
CHEEK](https://image.slidesharecdn.com/softtissuemorphology-180622062945/85/Soft-tissue-morphology-26-320.jpg)















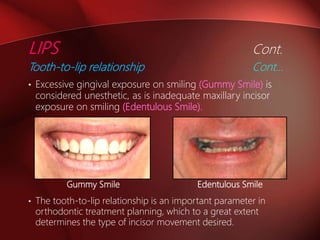
The document summarizes soft tissue morphology and behavior. It discusses how the lips, cheeks, tongue, and frenum can influence dental development through their forces and positioning. The lips have a molding effect on anterior teeth, while cheeks influence posterior teeth. An incompetent lip may cause malalignment through adoptive postures to maintain oral sealing. An enlarged tongue can procline teeth, while a small tongue allows arch narrowing. Abnormal frenum can cause diastemas. Soft tissues play an important role in guiding proper dental alignment.



































































