Downloaded 364 times
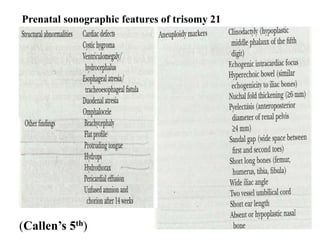
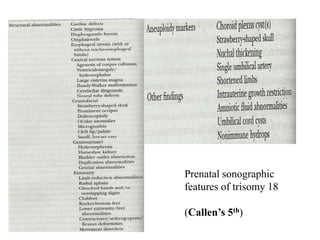
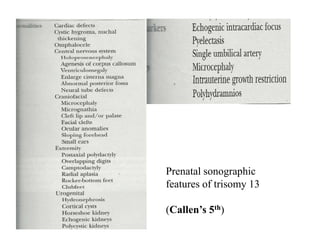
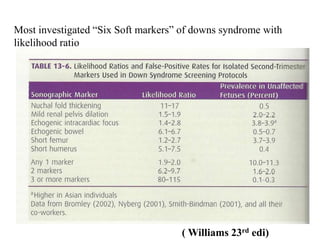
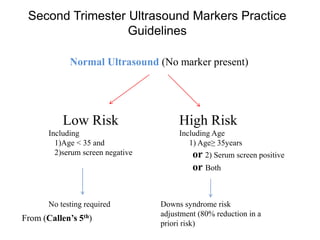
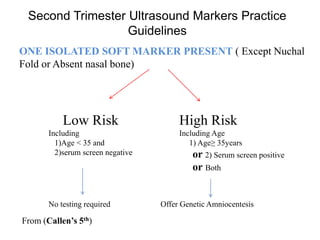
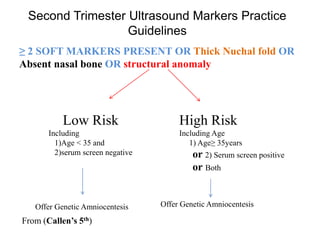
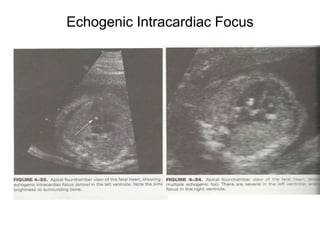
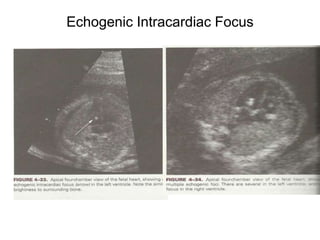
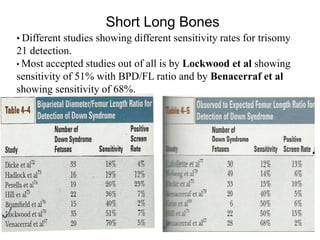
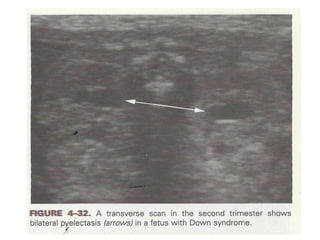


This document discusses various soft tissue markers that can be detected on a genetic sonogram to screen for fetal aneuploidies like Down syndrome. It describes markers like nuchal fold thickness, absent nasal bone, echogenic intracardiac focus, choroid plexus cysts, short long bones, pyelectasis, and single umbilical artery. It provides details on the sensitivity and significance of each marker, as well as guidelines on when genetic amniocentesis is recommended based on the number and type of markers present. The document emphasizes that while these markers can help detect aneuploidies, they are often transient and nonspecific findings that also occur commonly in euploid fetuses.























































































