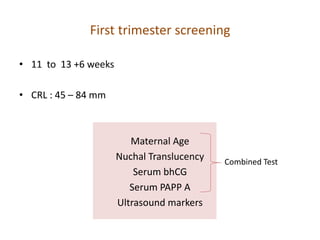
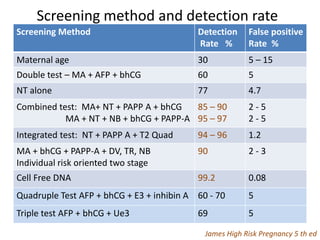
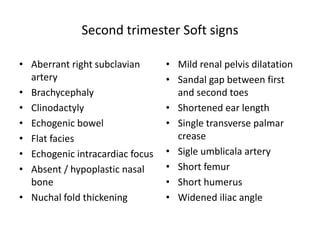
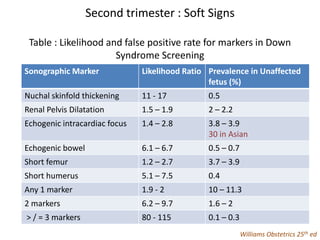
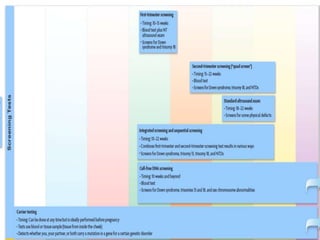
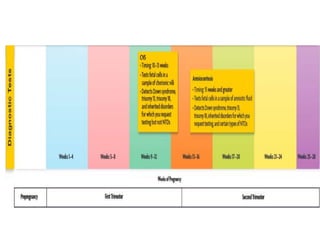
This document discusses prenatal genetic testing, including screening and diagnostic tests. It begins with an introduction to genetic testing during pregnancy. The first part focuses on various screening tests that can be done during the first and second trimester, including biochemical markers from blood tests and ultrasound examinations to measure factors like nuchal translucency. Later sections cover diagnostic tests, both invasive and non-invasive, as well as newer tests. The aim of prenatal genetic testing is to determine if genetic disorders are present and allow parents to make informed choices.