Download as PDF, PPTX

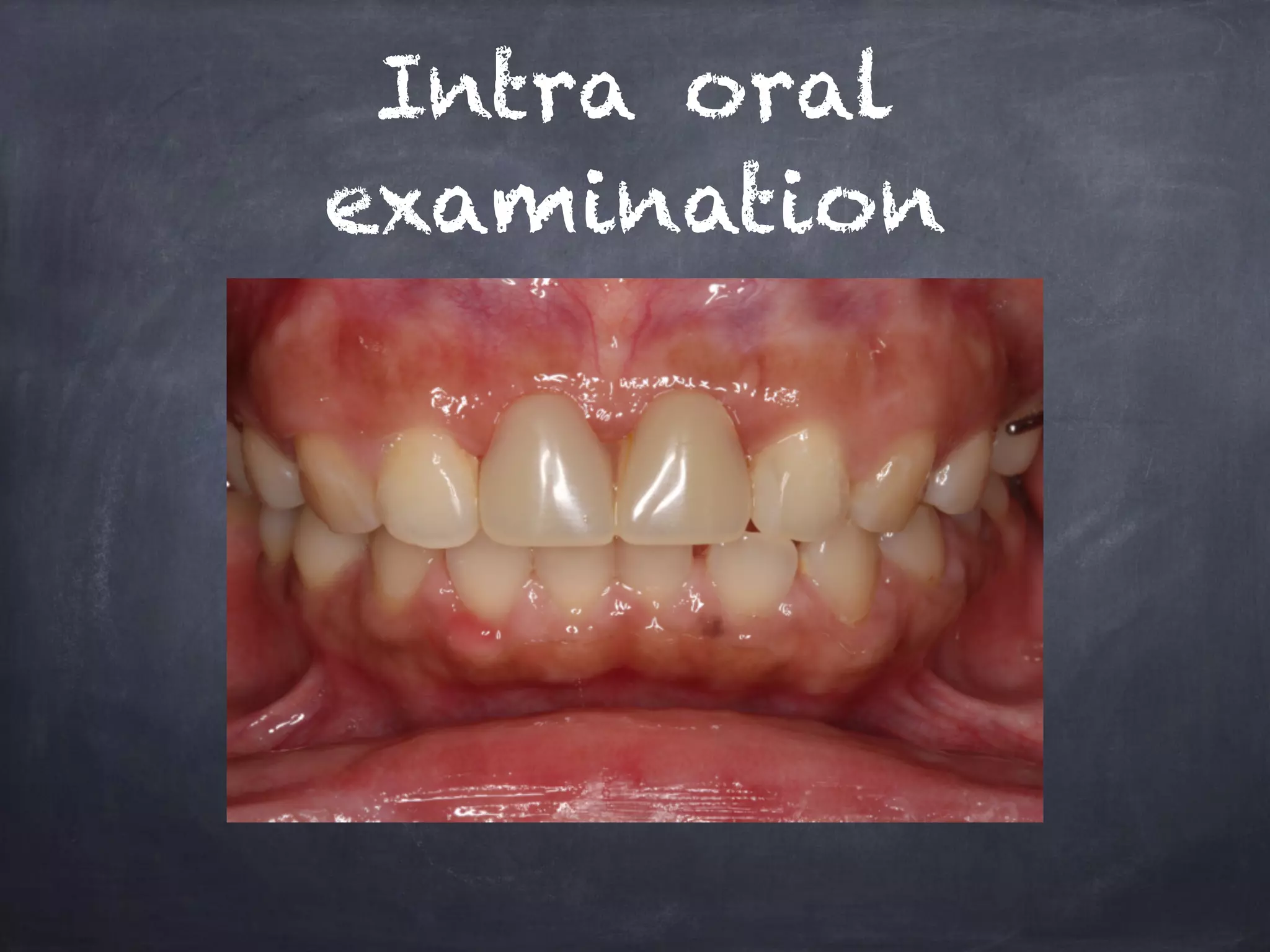
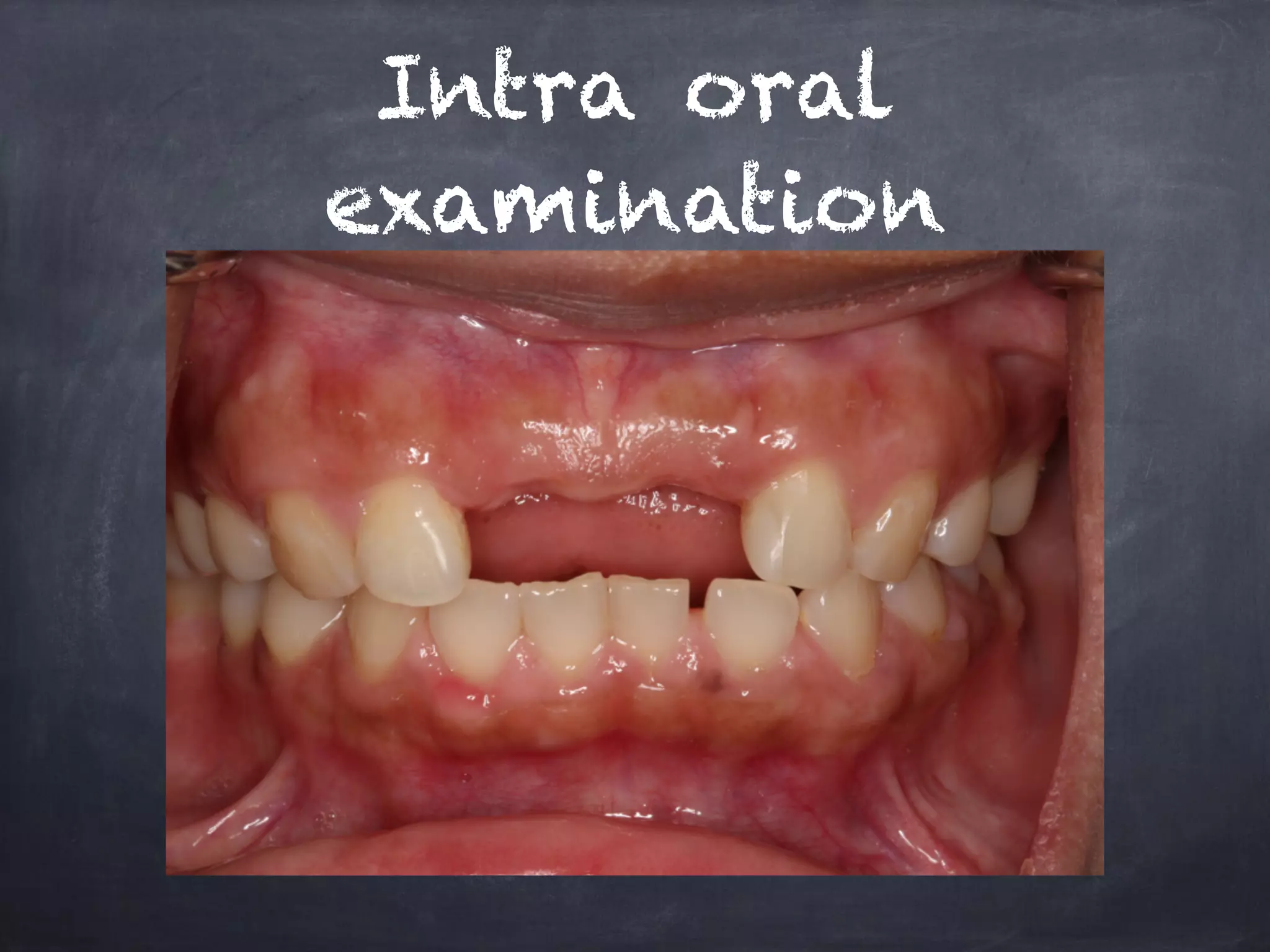
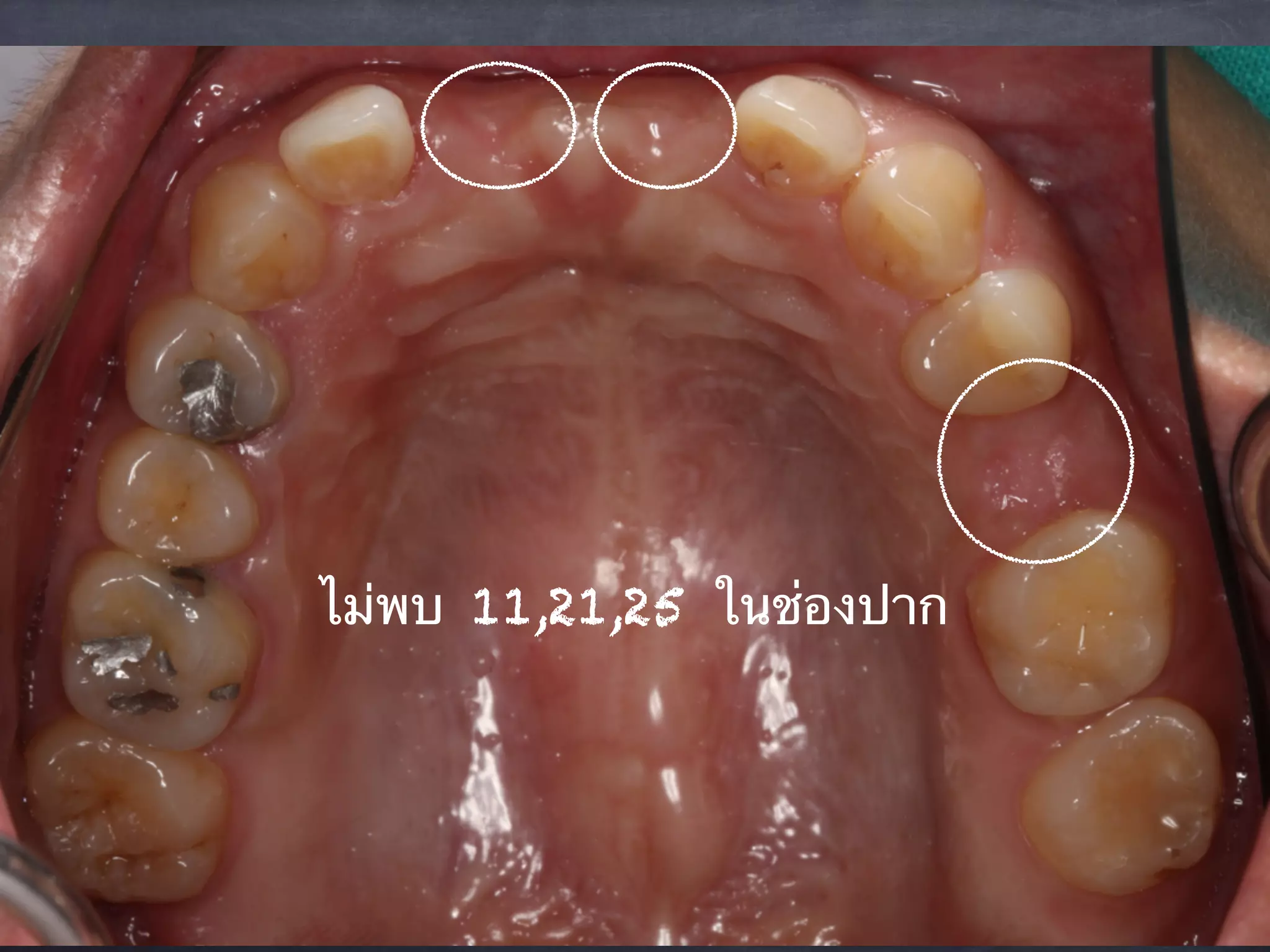

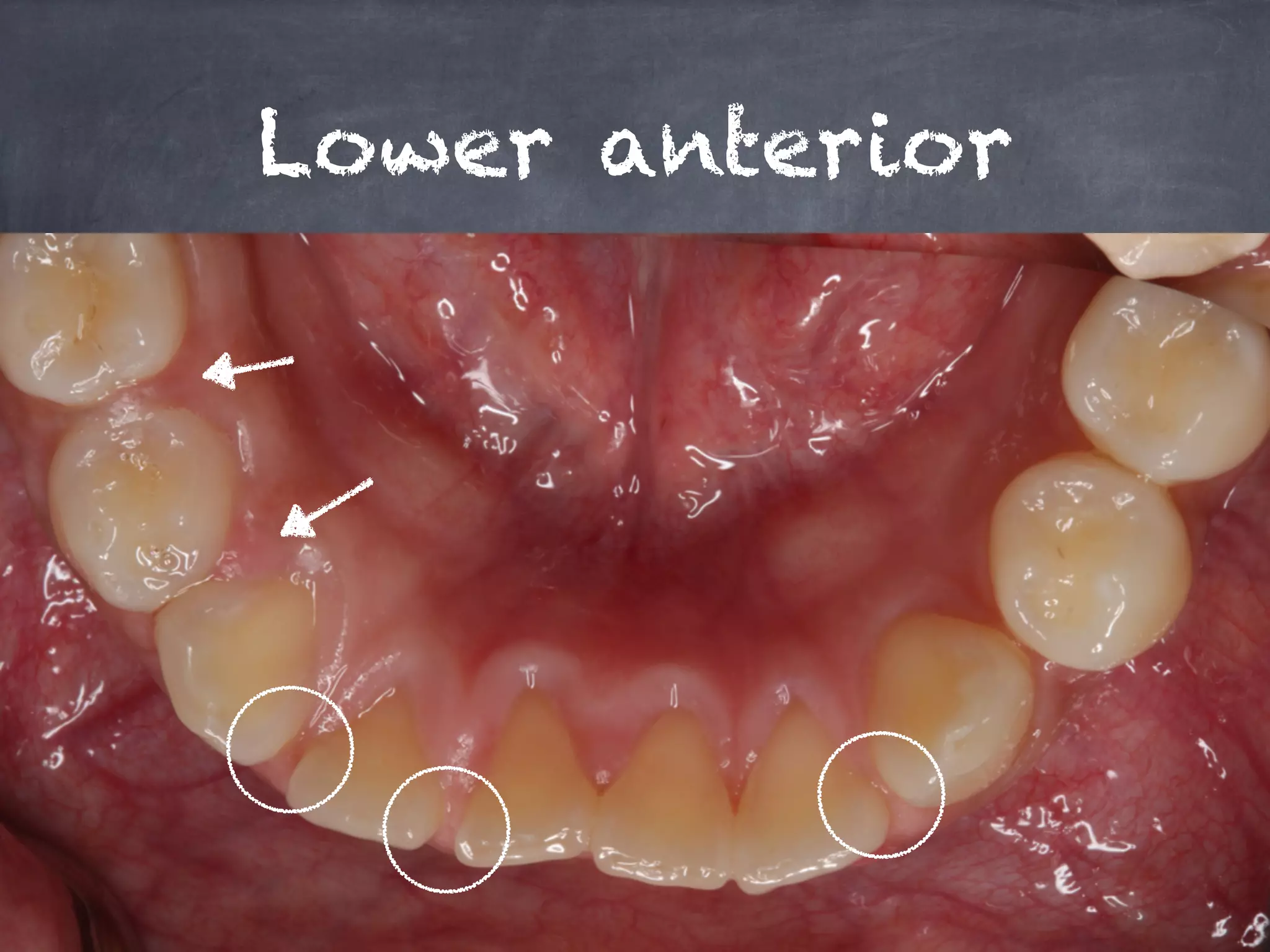




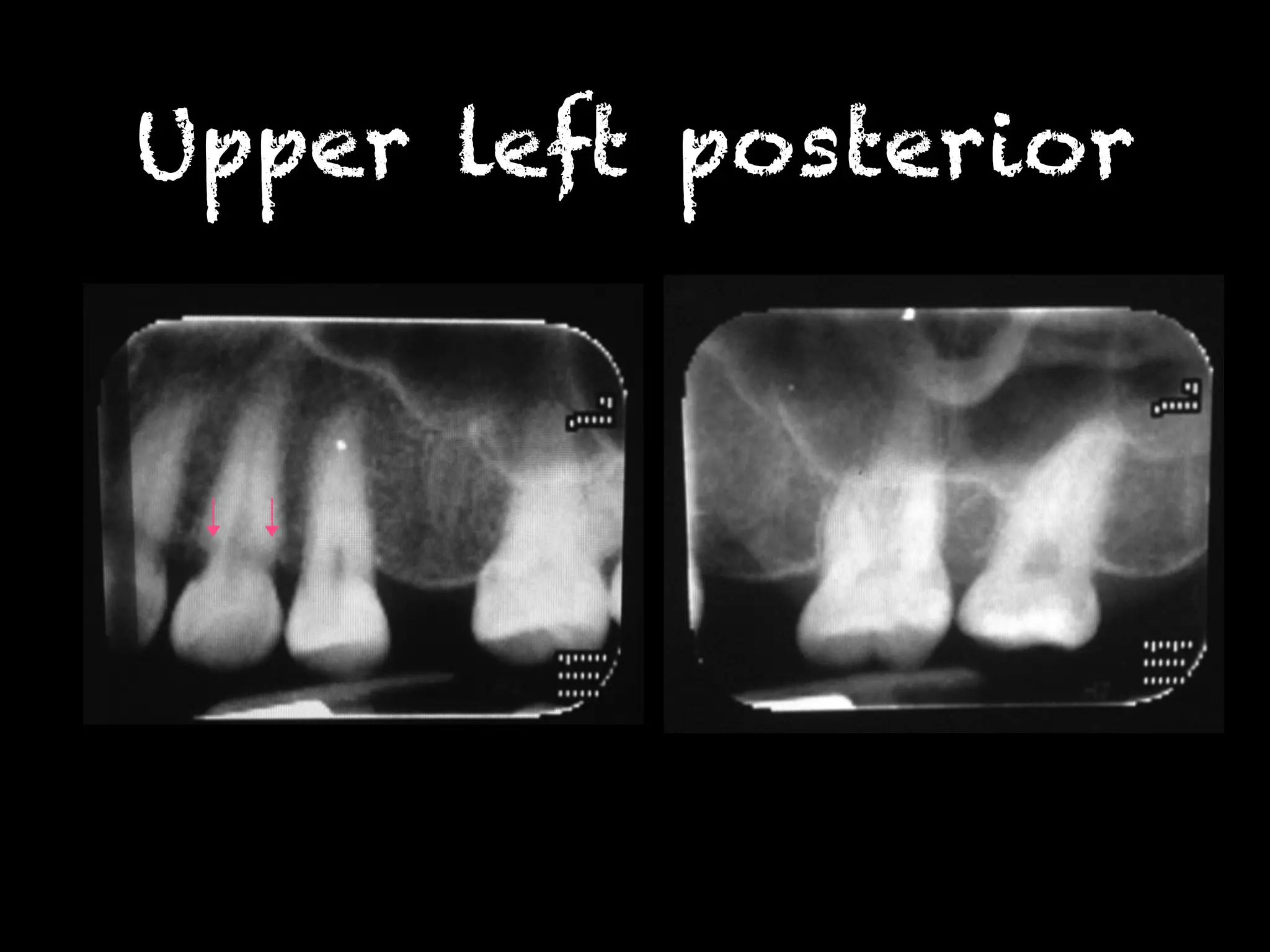
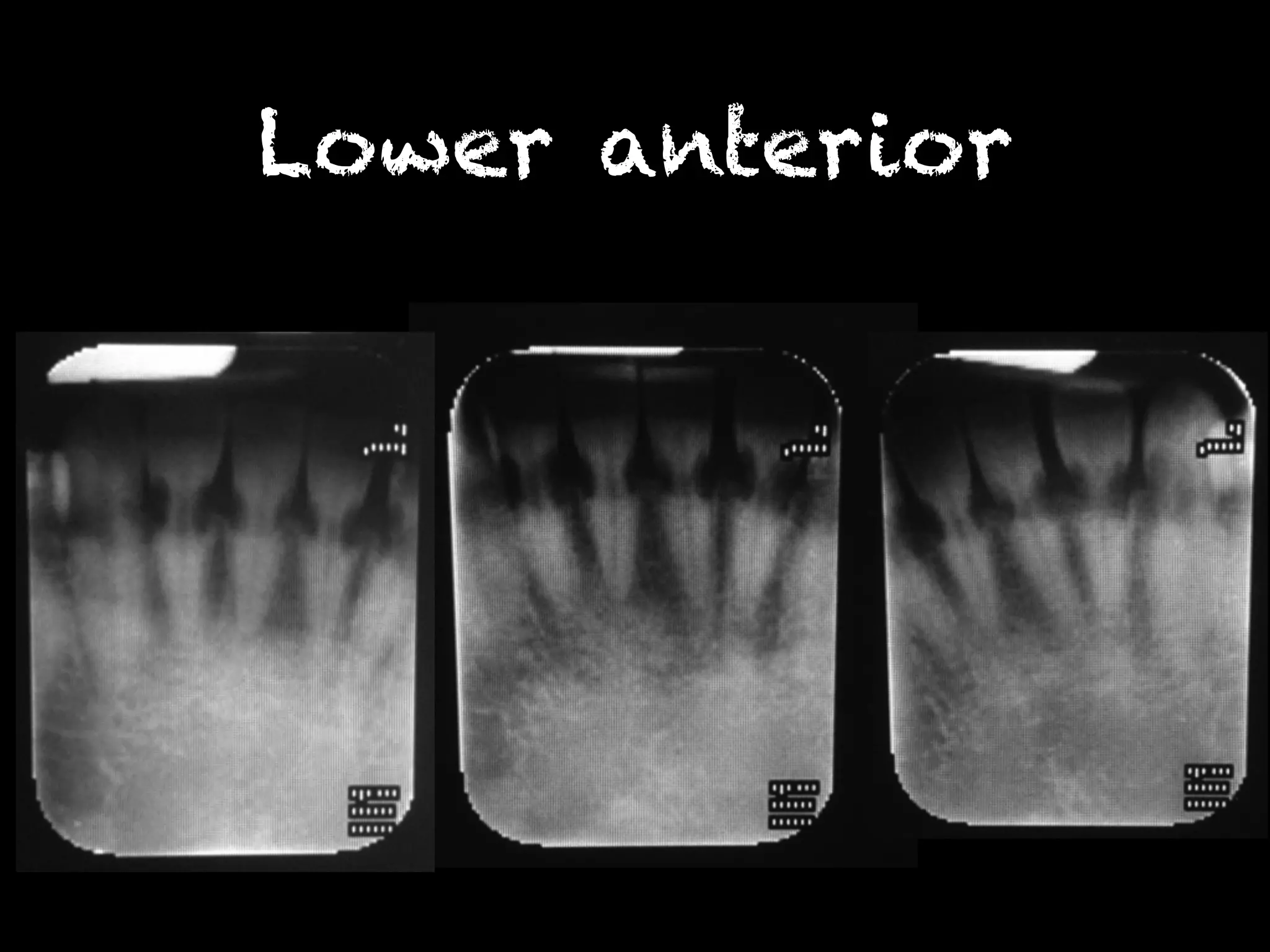

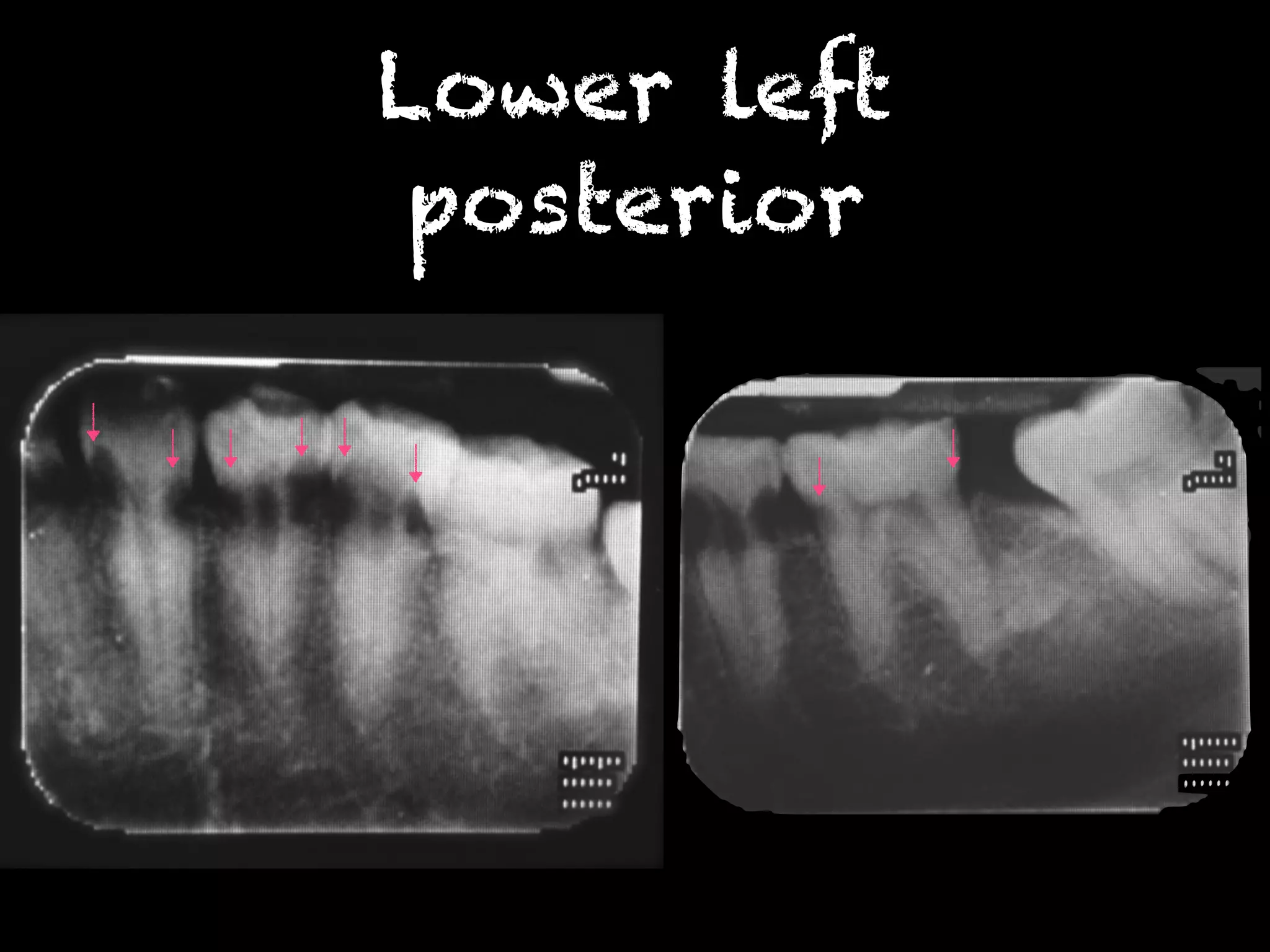

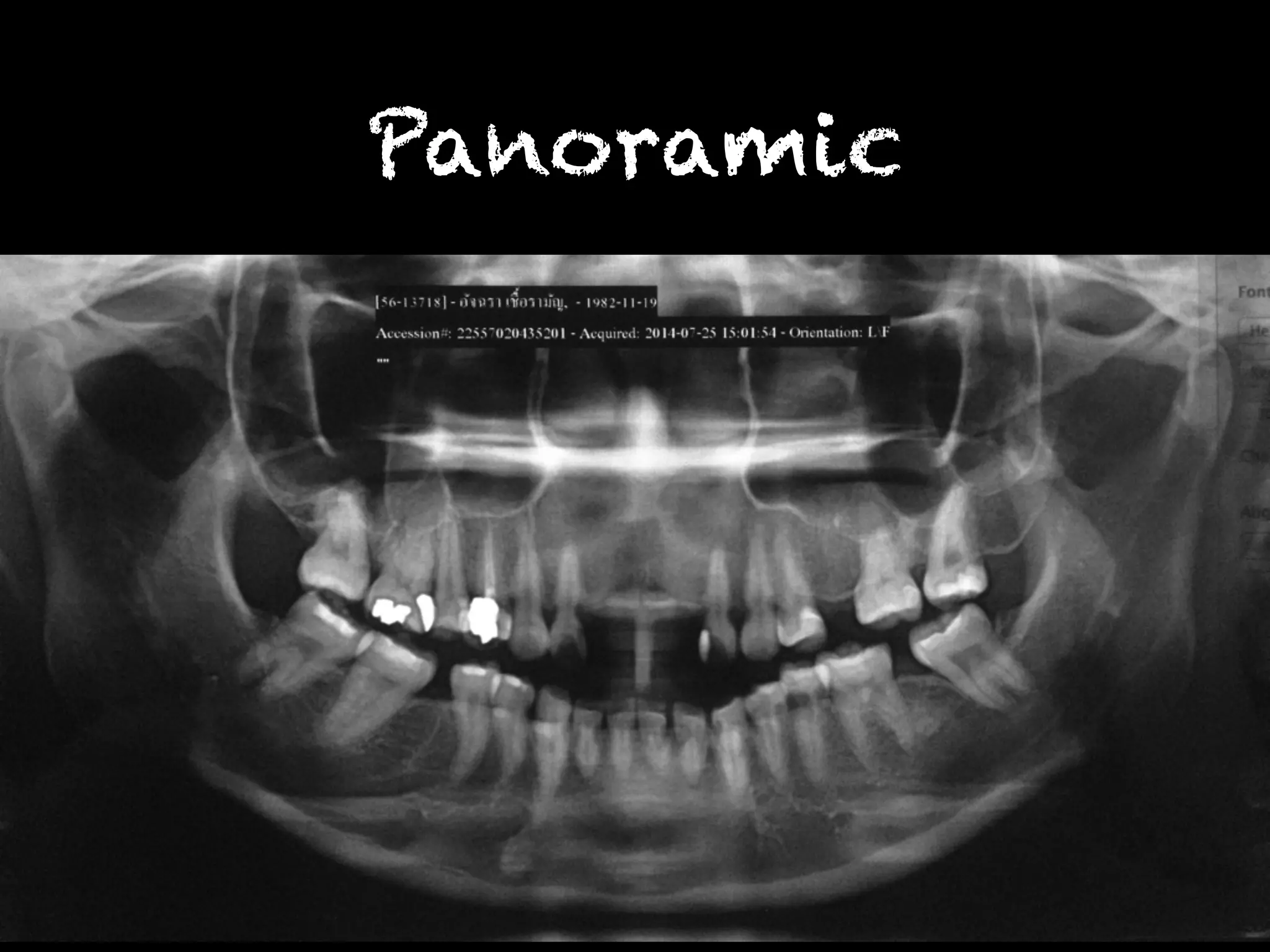
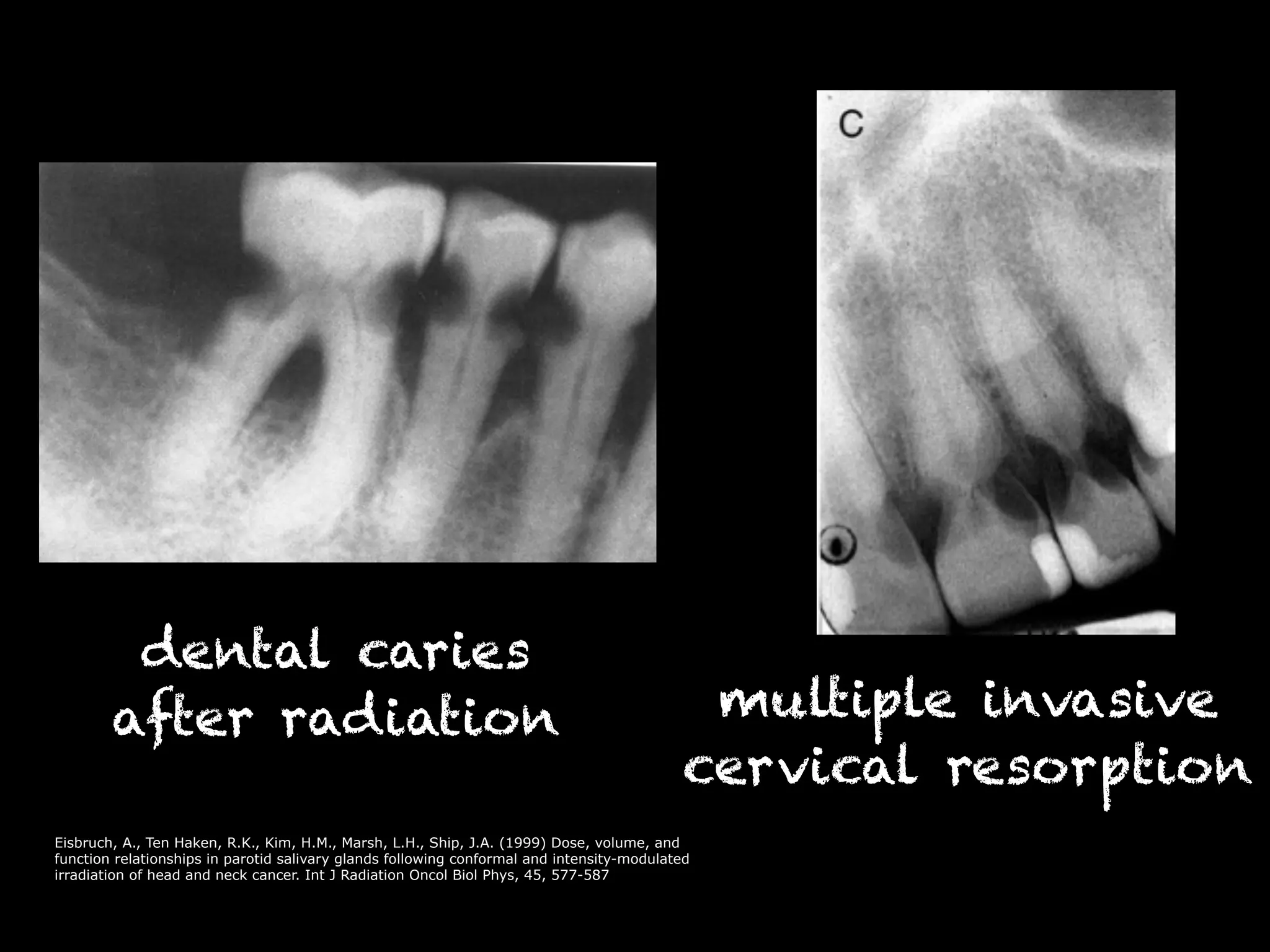


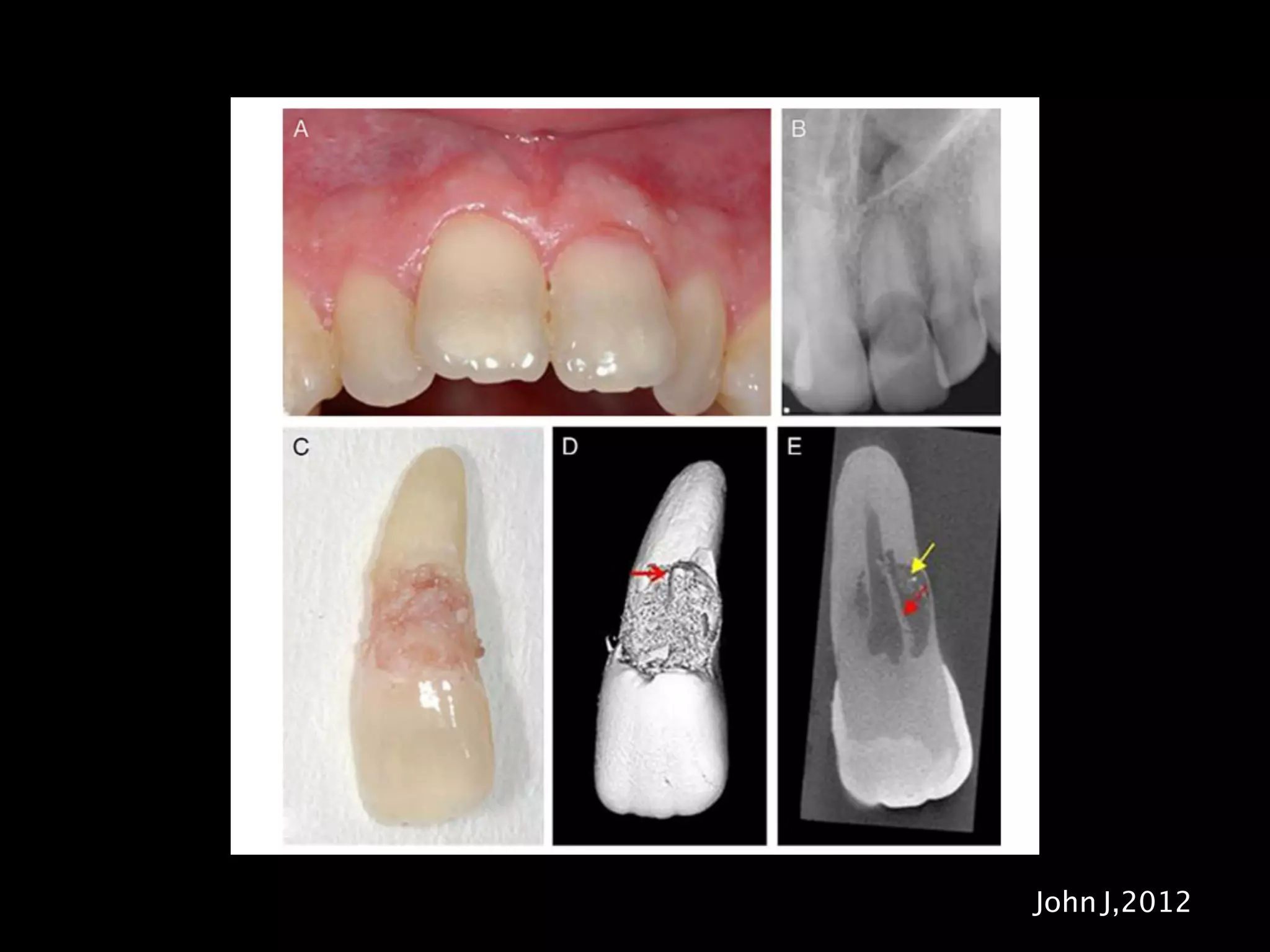
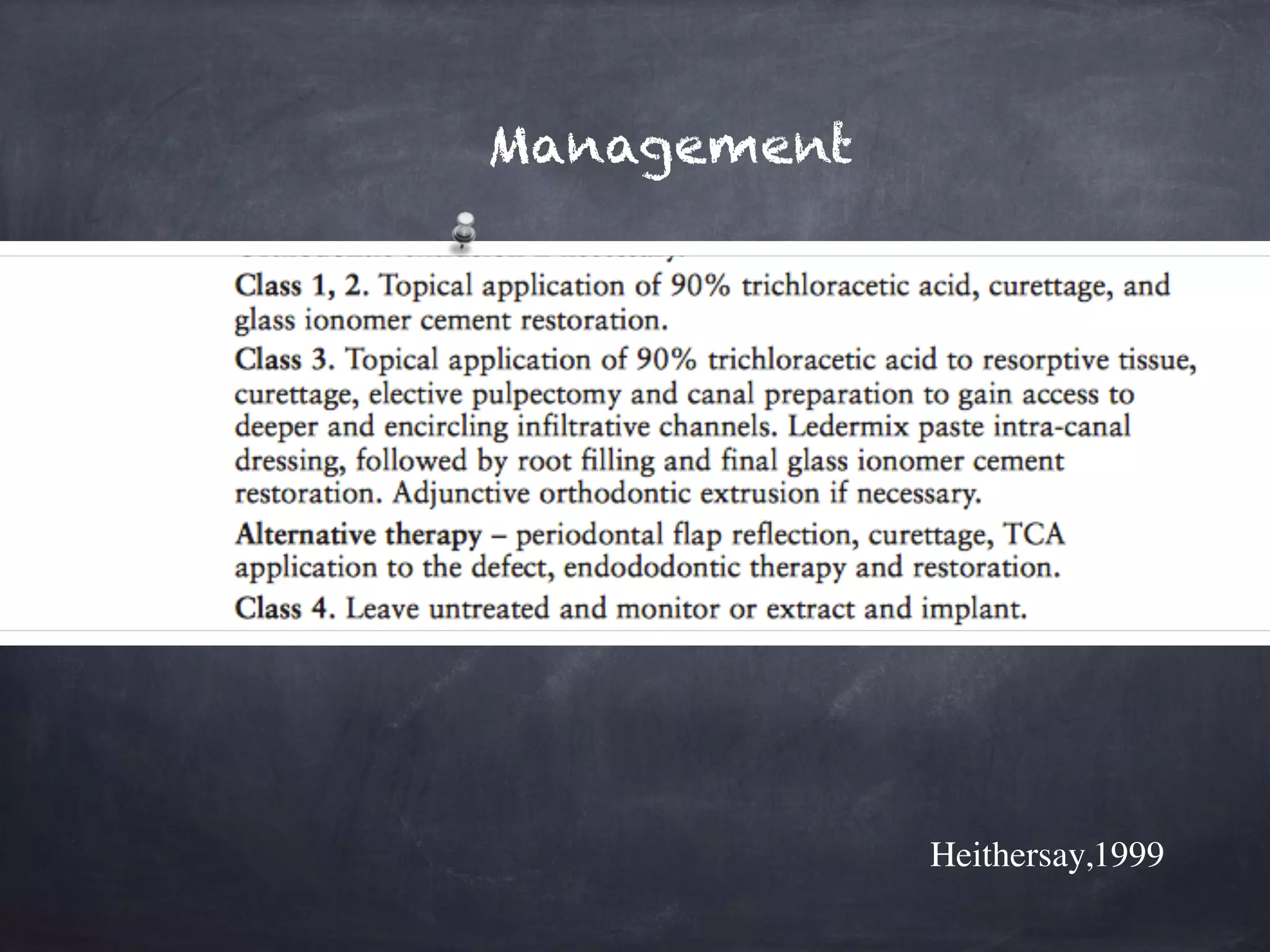
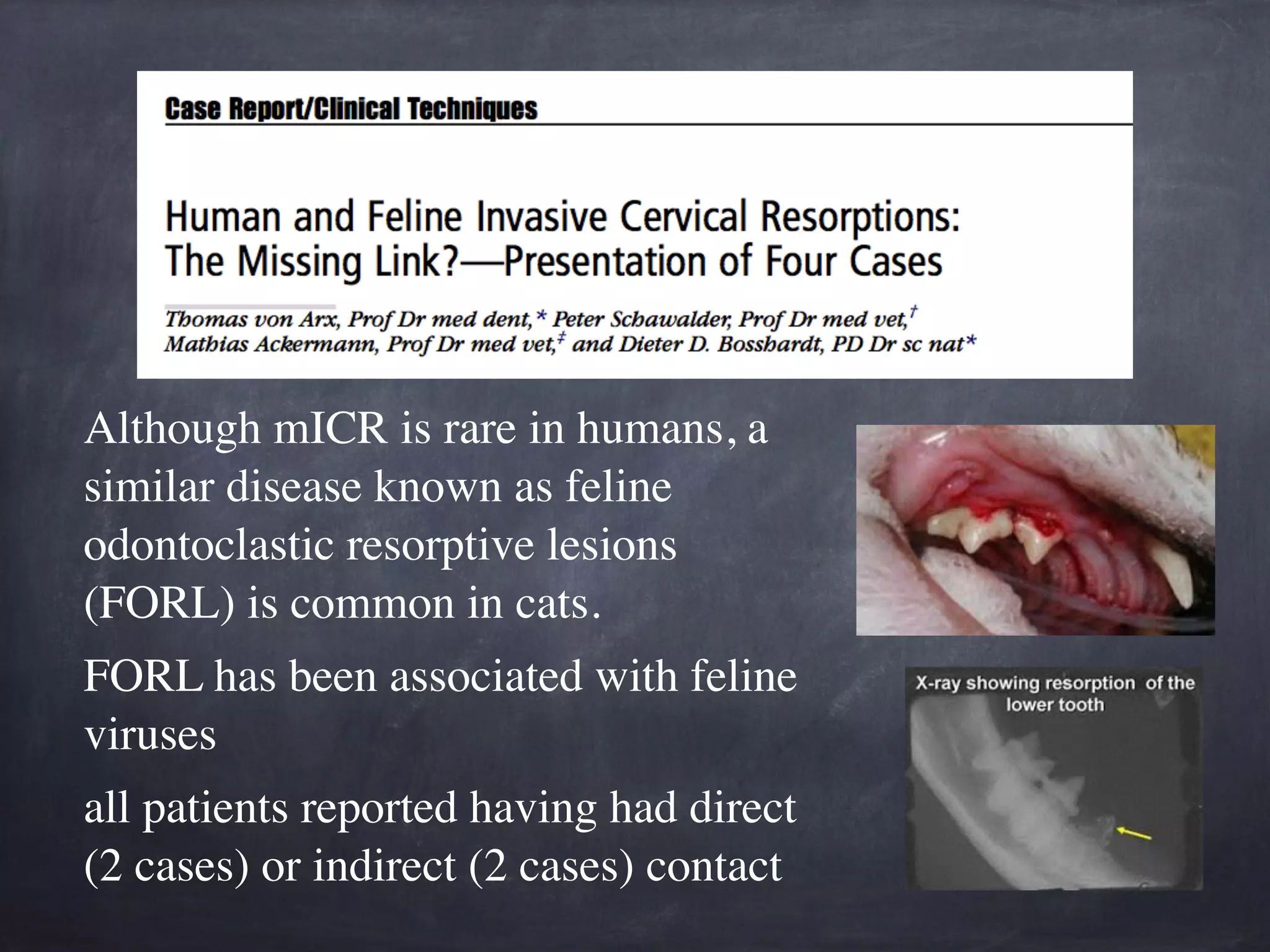
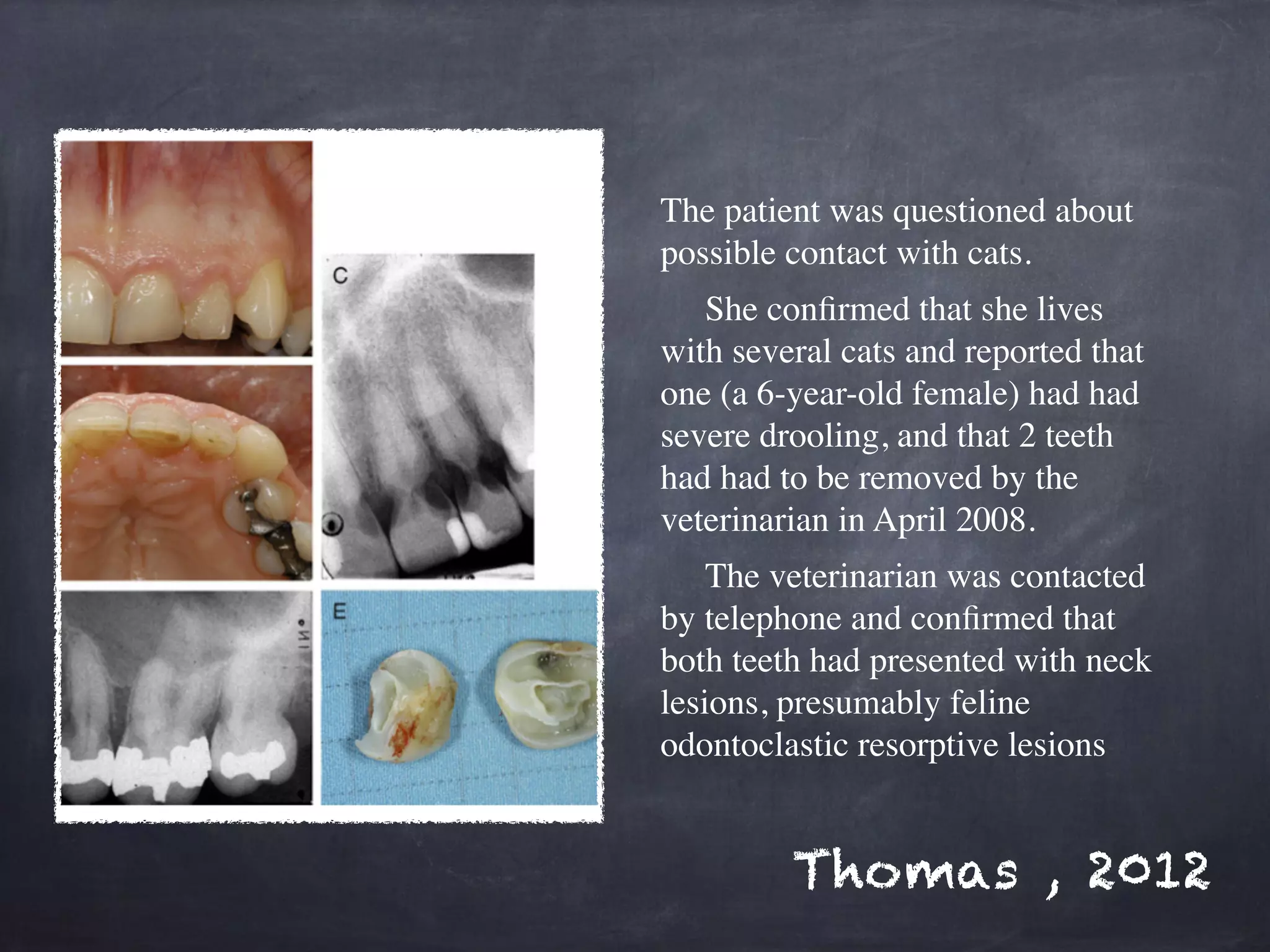
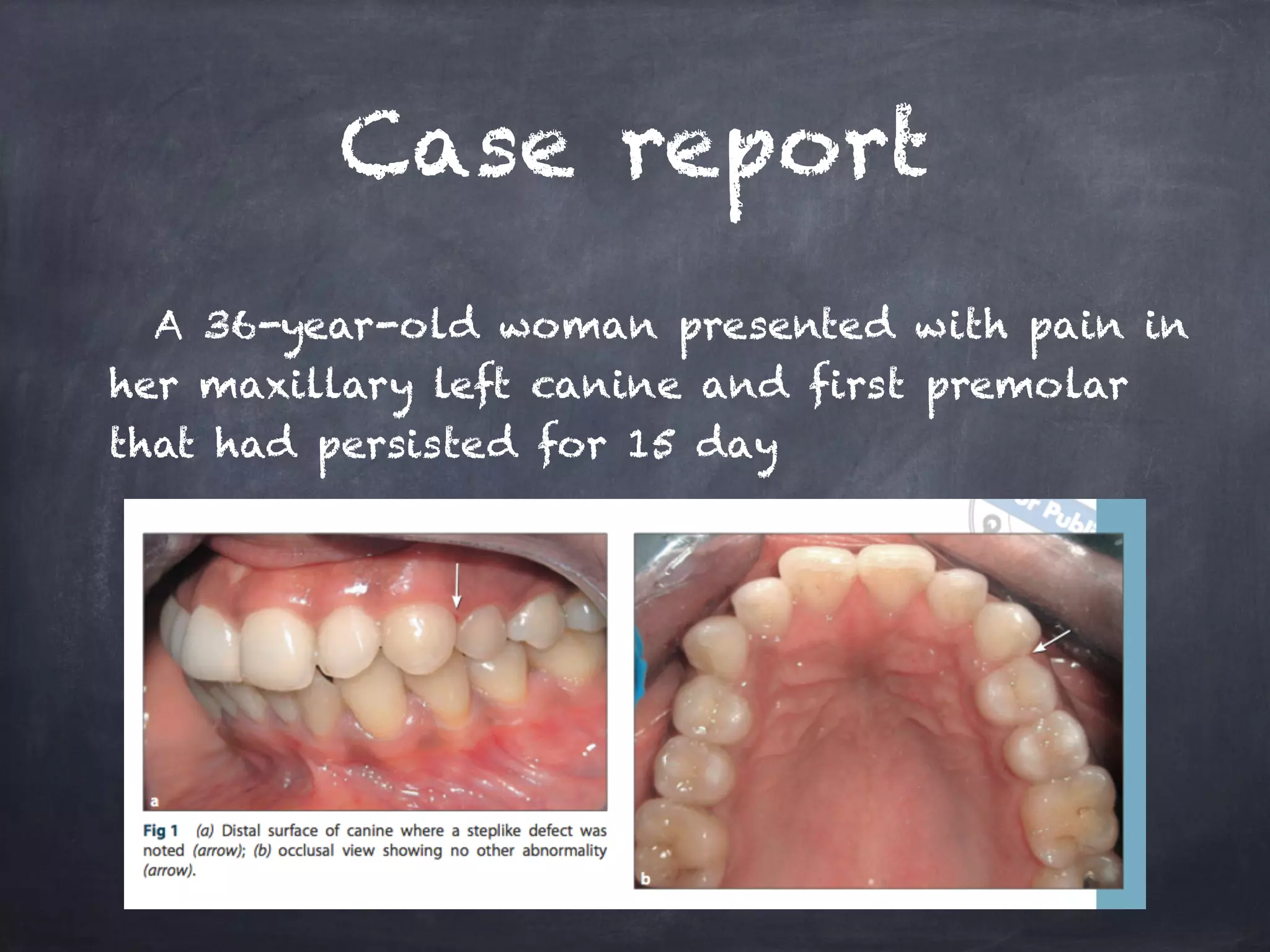
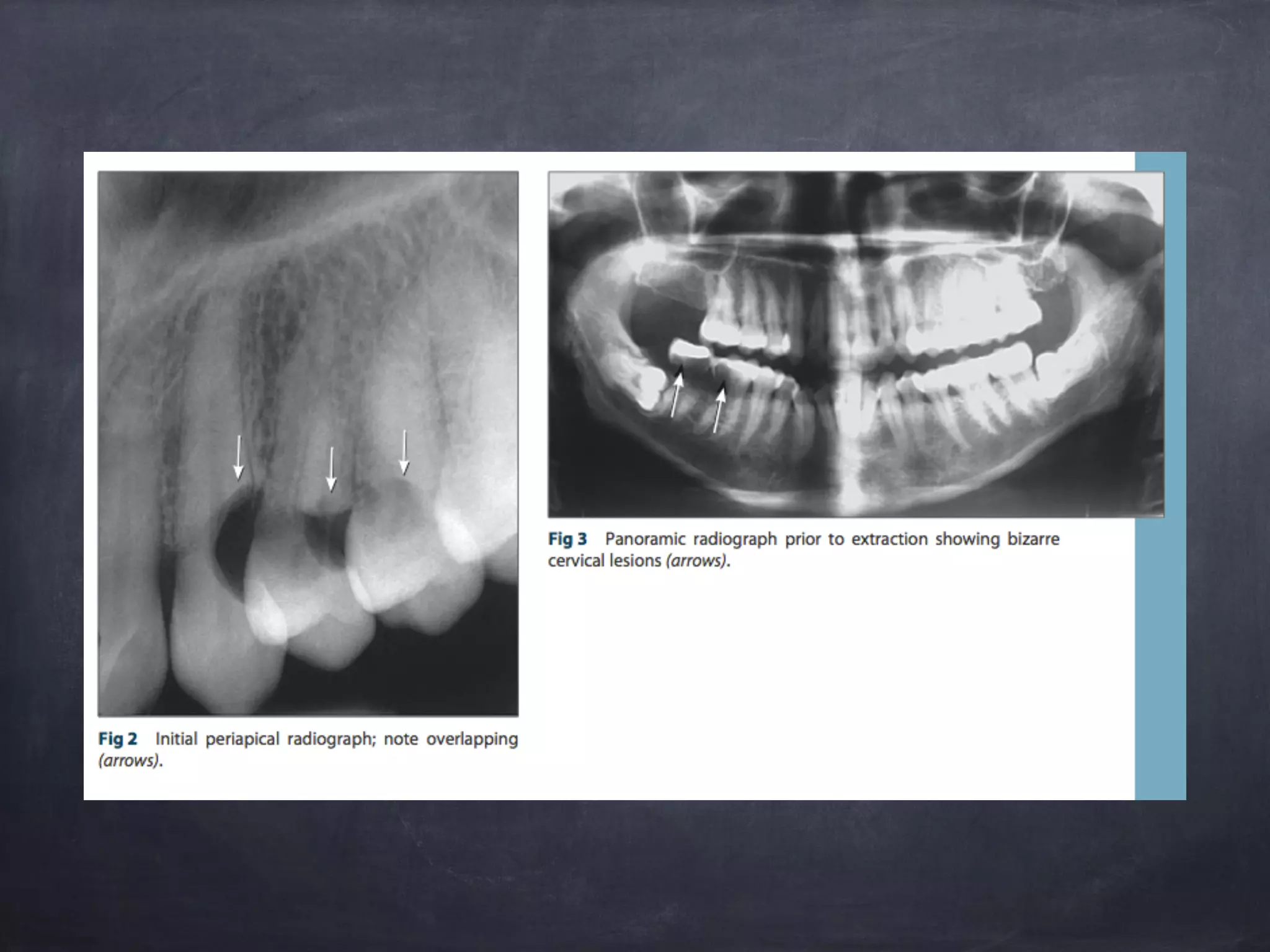
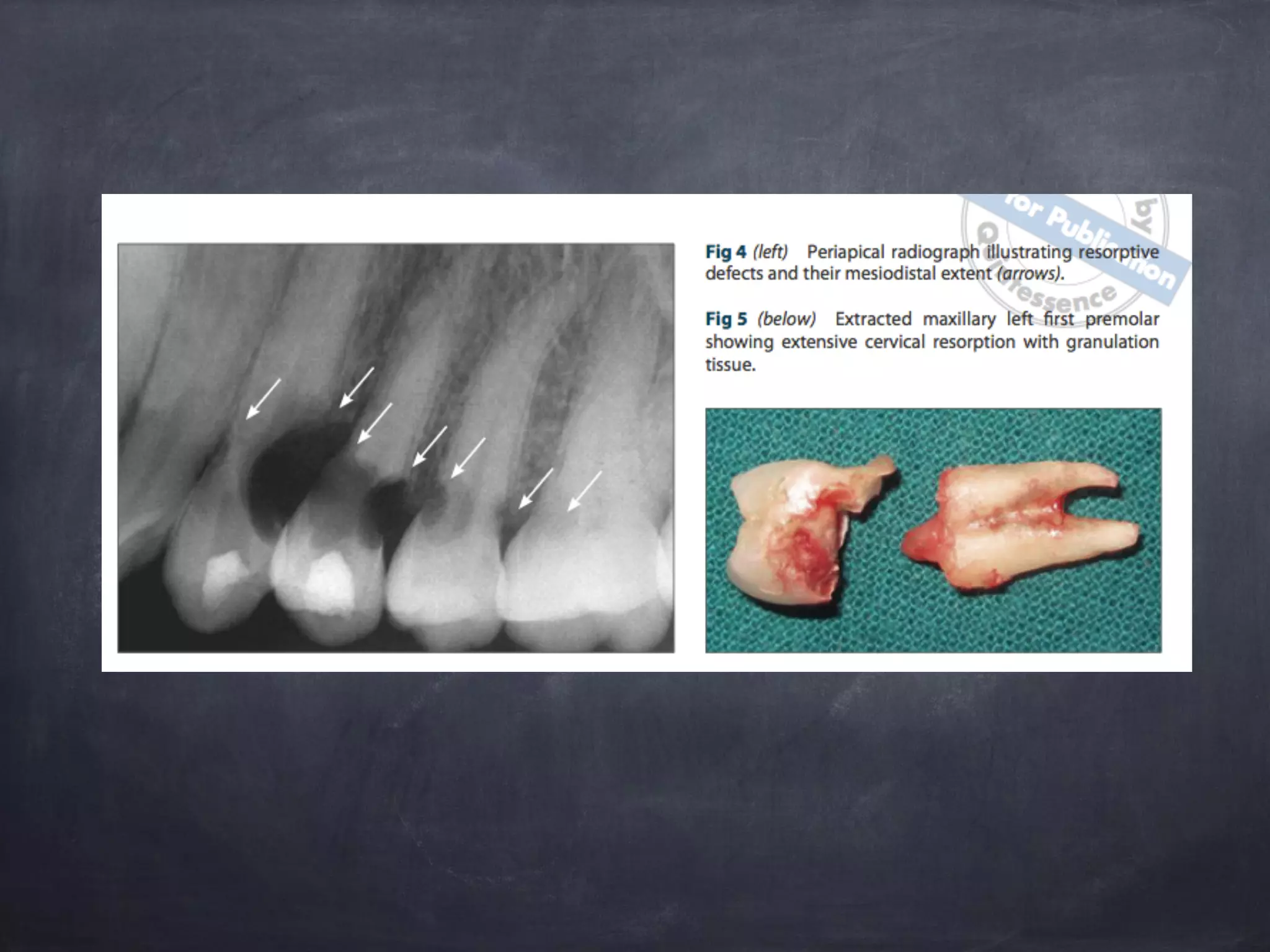
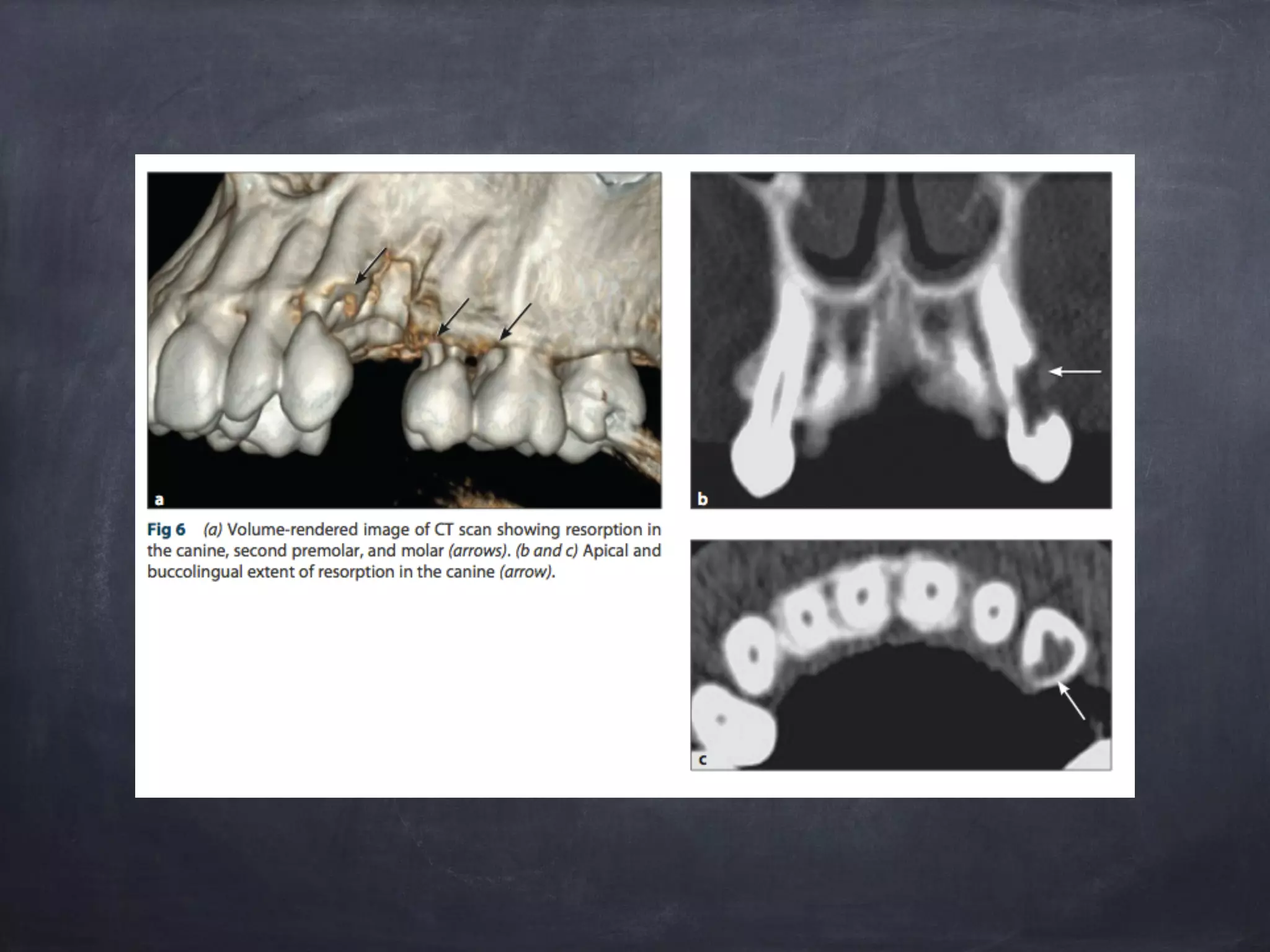
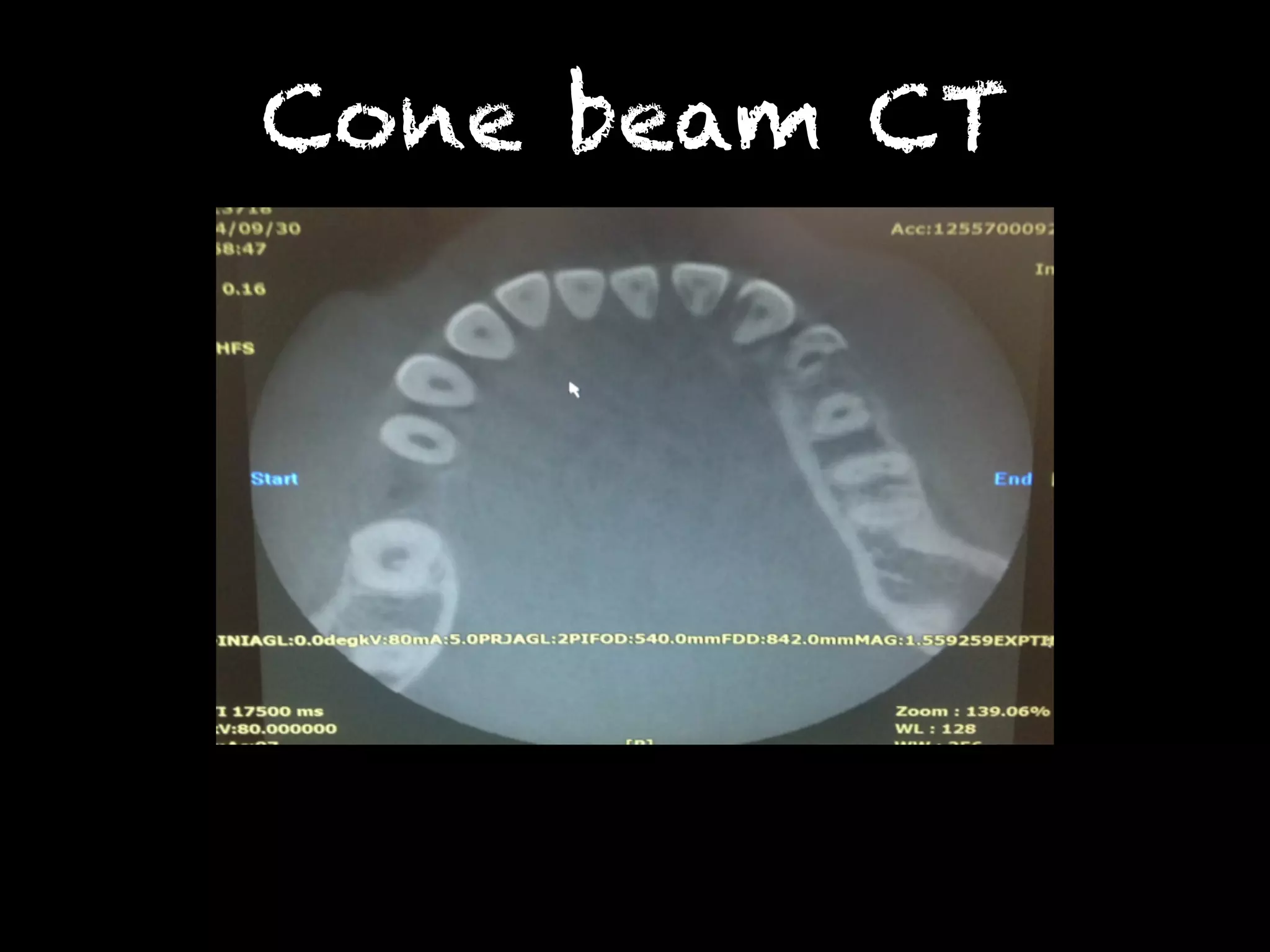
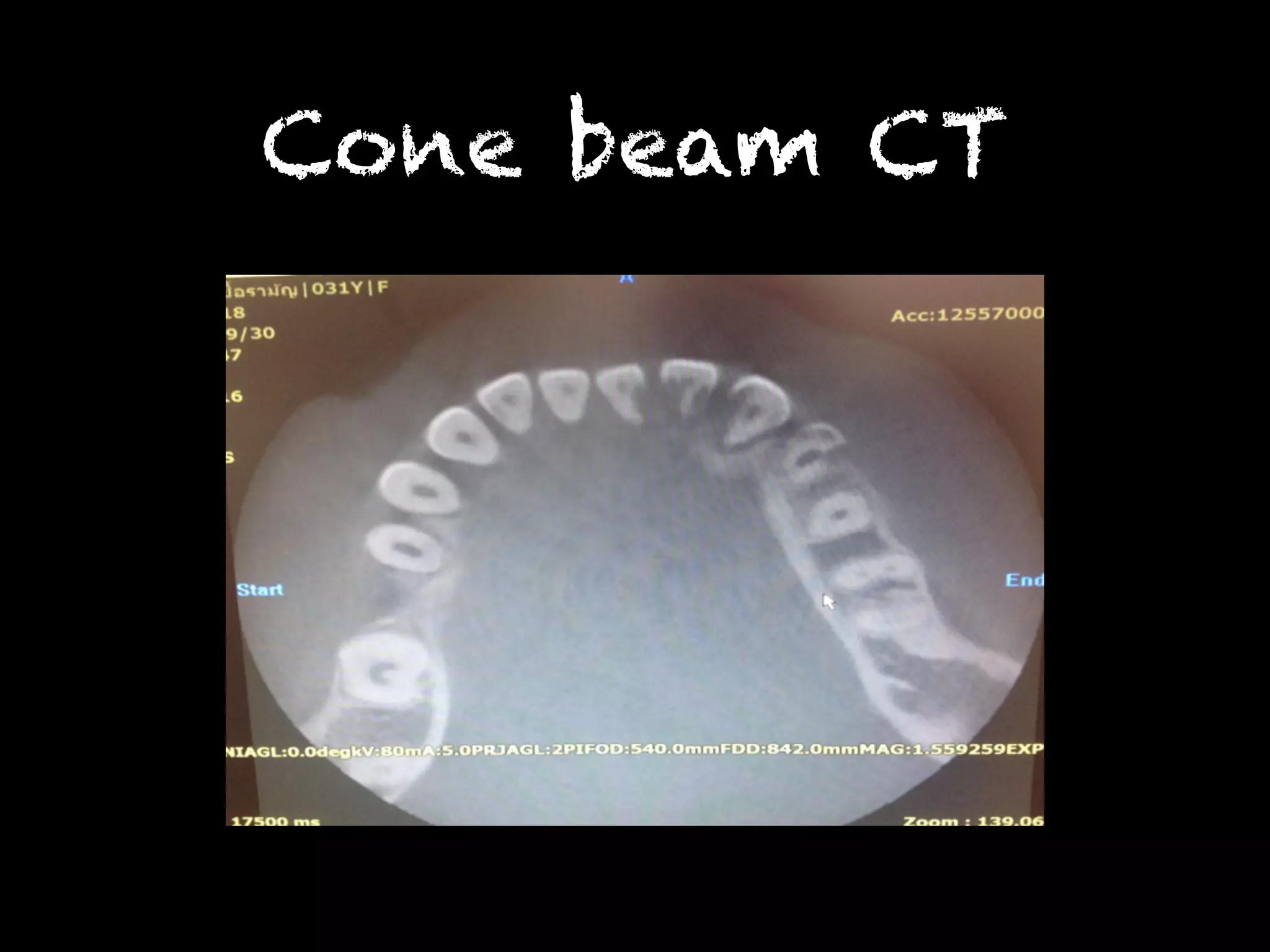
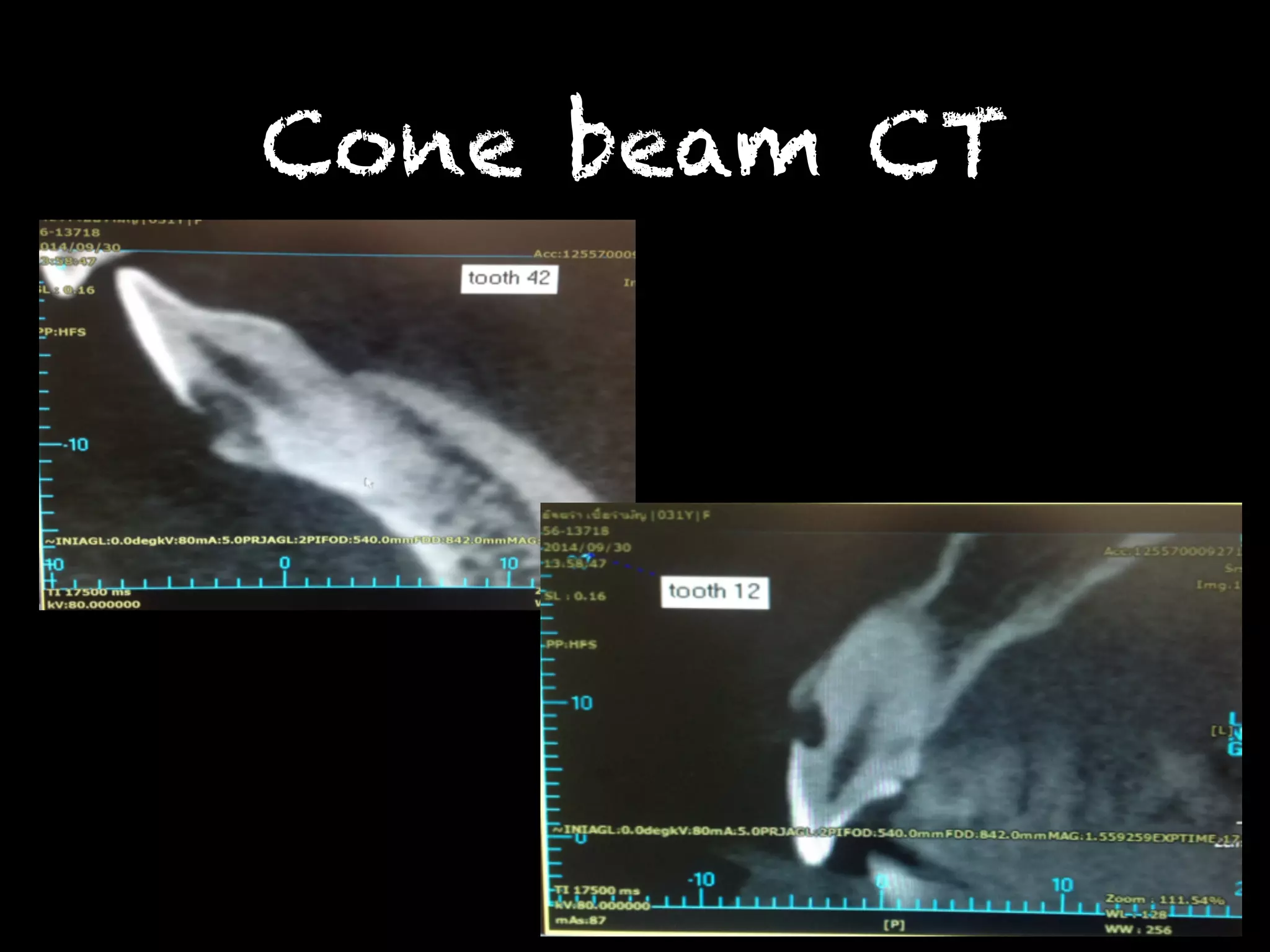
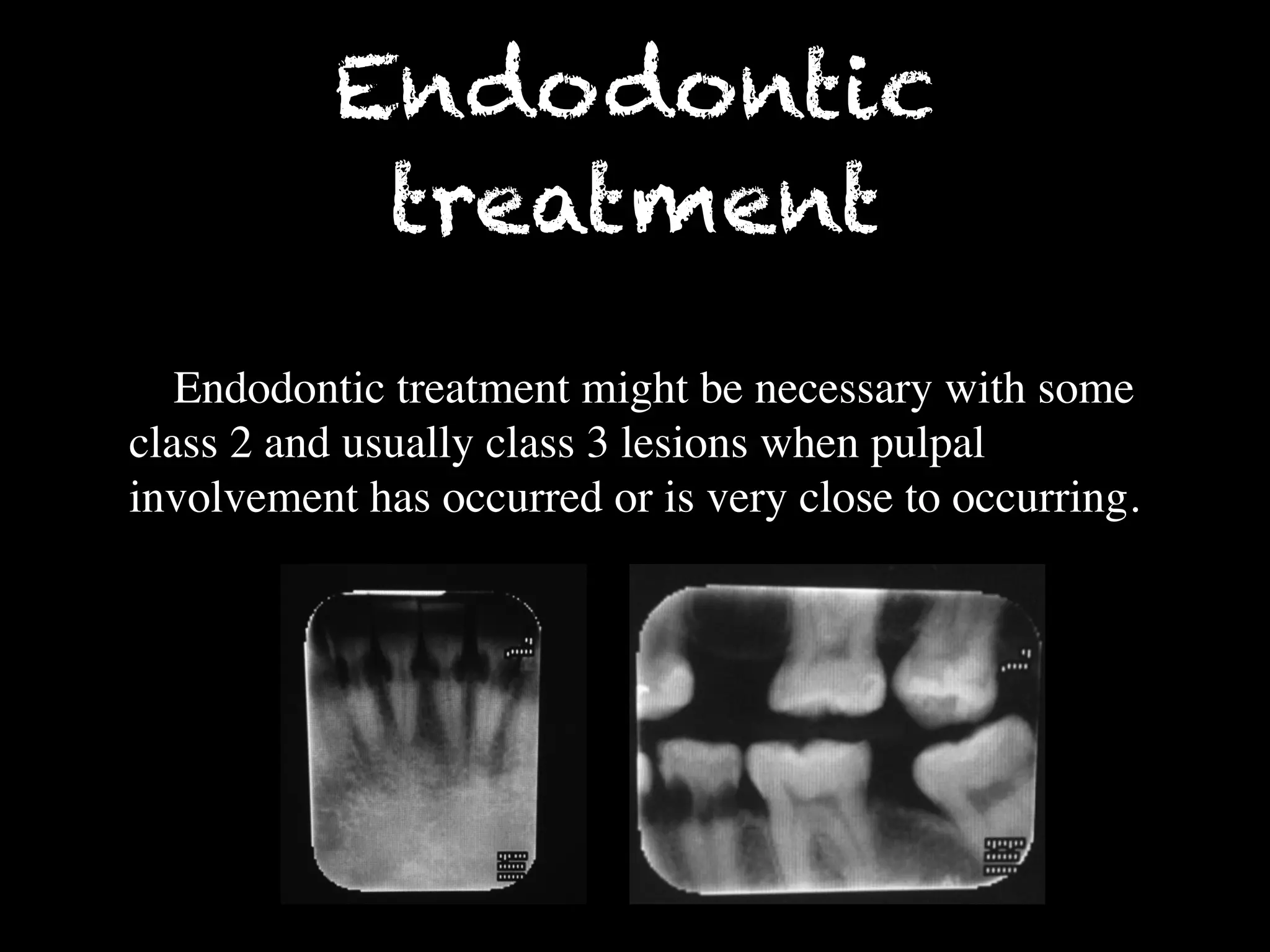



This document summarizes a dental case conference regarding a 31-year-old female patient presenting with multiple invasive cervical resorptions. Examination found lesions on several teeth. The differential diagnosis included dental caries and root resorption. Further radiographic examination and consultation with a radiologist supported a diagnosis of multiple invasive cervical resorption. This type of resorption is rare in humans but similar to a condition seen in cats caused by feline viruses. The patient confirmed contact with cats, one of which had recent dental issues, supporting possible transmission of a virus. Treatment options for this condition were discussed.























































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)











