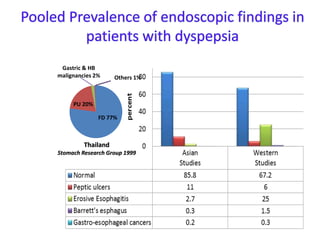
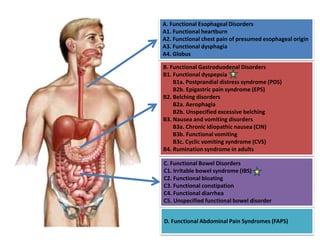
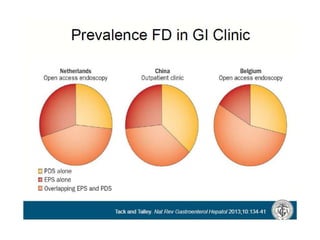
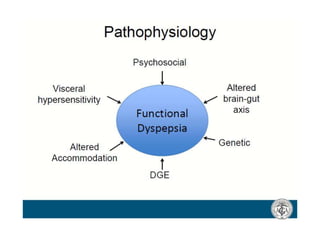
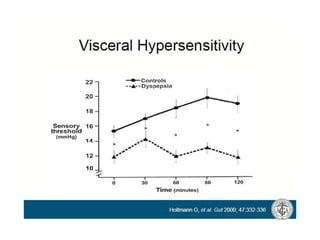
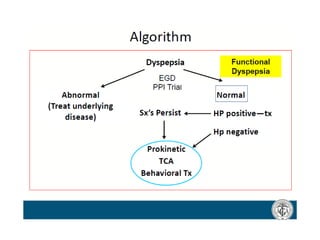
Functional dyspepsia is a common chronic gastrointestinal condition characterized by chronic upper gastrointestinal symptoms like indigestion, discomfort, early satiety, and bloating without structural abnormalities. It has a substantial impact on quality of life. The underlying causes can include GERD, peptic ulcer disease, infections, lactose intolerance, medications, and functional (non-ulcer) dyspepsia. Treatment options include acid suppressants, prokinetics, Helicobacter pylori eradication in infected patients, and complementary and alternative therapies. Empirical treatment is justified in typical cases without alarm symptoms, and treatment should be tailored based on the patient's most bothersome symptom.





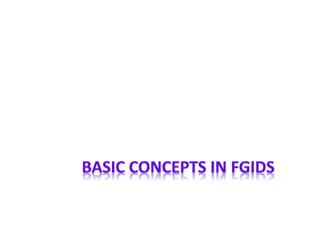

![• 1 Trial, 109 patients
• 1.02 [0.76, 1.36]
Antacids
• 13 Trials, 3179 patients
• 0.67 [0.55, 0.82]
Prokinetics
• 12 Trials, 2183 patients
• 0.77 [0.65, 0.92]
H2RA
• 1 Trial, 40 patients
• 0.32 [0.13, 0.79]
Misoprostol
• 2 Trials, 163 patients
• 0.50 [0.31, 0.81]
Antimuscarinics
• Non significant different
Bismuth & Sucralfate
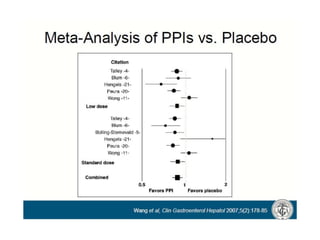
Outcome: Global Symptoms Assessment at end of treatment
Moayyedi P., et al. The Cochrane Library 2007, Issue 3](https://image.slidesharecdn.com/funtionaldyspepsiaemail-240315023731-78da83aa/85/Funtional-Dyspepsia-GIT-and-Liver-power-point-41-320.jpg)
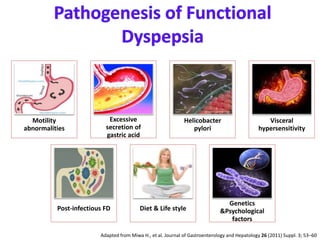
![Outcome title # of studies # of participants Effect size [95%CI]
GSA (D) 10 3347 0.87 [0.80, 0.96]
QoL score 3 1630 0.21 [-1.66, 2.09]
GSA (C) 5 1894 -0.12 [-0.22, -0.02]
Comparisons Outcome # of studies # participants Effect size [95%CI]
PPI vs H2RA GSA 2 739 0.93 [0.84, 1.02]
Half vs full dose
PPI
GSA 6 2032 0.98 [0.92, 1.04]
Moayyedi P., et al. The Cochrane Library 2007, Issue 3
GSA=Global Symptom Assessment, QoL=Quality of Life](https://image.slidesharecdn.com/funtionaldyspepsiaemail-240315023731-78da83aa/85/Funtional-Dyspepsia-GIT-and-Liver-power-point-43-320.jpg)
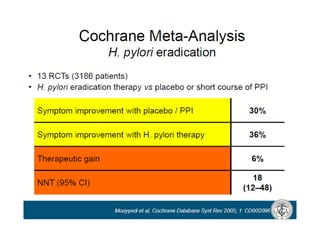
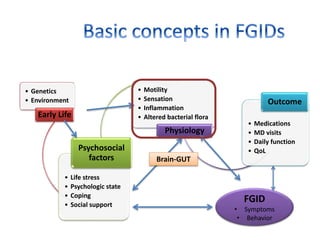
![Moayyedi P,et al. The Cochrane Library 2006, Issue 3
• Global symptom scores between 3-12 months F/U
• 17 studies, 3566 subjects
• HP eradication has small but significant better outcome than placebo
• Relative Risk (Fixed) 0.90 95% CI [0.86, 0.94] – favor HP eradication
• The NNT to cure one case of dyspepsia = 14 (95% CI = 10 to 25)](https://image.slidesharecdn.com/funtionaldyspepsiaemail-240315023731-78da83aa/85/Funtional-Dyspepsia-GIT-and-Liver-power-point-46-320.jpg)
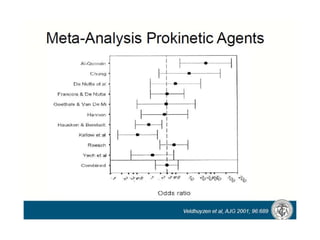
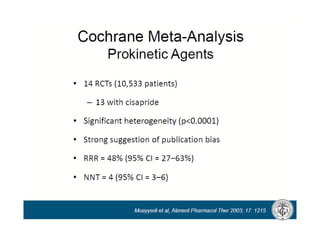
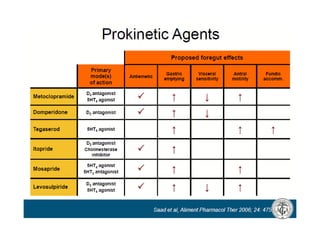
![Studies:
• Prokinetics: metoclopramide, domperidone, trimebutine, cisapride, itopride and mosapride,
used for Rx of FD between 1951 and 2005.
• 27 studies were selected. 1844 in an experimental arm, 1591 in placebo arm
Outcomes
•Difference in the probability of response of the interventional drug VS placebo.
•Heterogeneity: Meta-regression analysis.
•Publication bias: funnel plot and statistical testing (P = 0.975).
•The summary statistic was 0.295[0.208-0.382, P < 0.001]
•the interventional drug has 30% excess probability of producing a response compared with placebo.
•The most significant source of heterogeneity was the year of publication (P < 0.001)
Conclusion:
•prokinetics are significantly more effective than placebo in the Rx of FD.
•efficacy was assessed over short periods.
•Long-term randomized controlled trials are needed to confirm the effect.
Hiyama T., et al. J Gastroenterol Hepatol 2007 Mar;22(3):304-10](https://image.slidesharecdn.com/funtionaldyspepsiaemail-240315023731-78da83aa/85/Funtional-Dyspepsia-GIT-and-Liver-power-point-47-320.jpg)






































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)







![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
