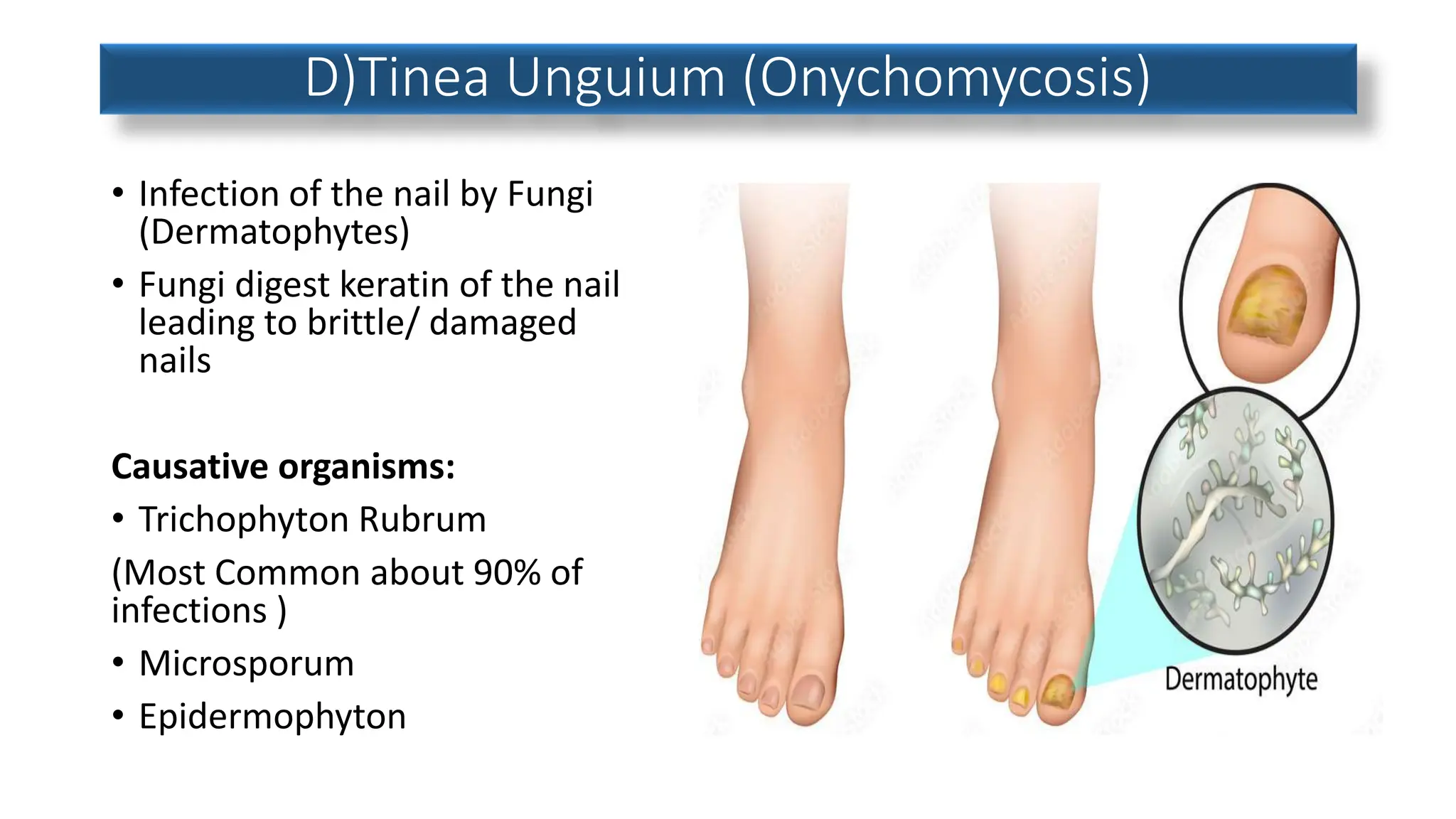
This document discusses various fungal infections affecting humans. It describes superficial infections like athlete's foot, ringworm, and jock itch which are caused by dermatophytes. Deep fungal infections that enter the body are also discussed. Common dermatophyte infections are described in detail including symptoms, transmission, risk factors and treatment. Pityriasis versicolor and vaginal yeast infections are also summarized. The document provides an overview of common fungal infections and dermatophytosis.































































![Fungal infections of skin [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/fungalinfectionsofskincompatibilitymode-130321223403-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)










































