Downloaded 441 times








Marjorie Gordon proposed 11 functional health patterns as a standardized approach to comprehensive nursing data collection. The patterns include health perception, nutrition, elimination, sleep, roles and relationships, sexuality, coping, and values. For each pattern, the nurse collects subjective and objective data to identify health issues and needs. Functional health patterns provide a systematic framework to assess all aspects of a person's health.
Introduces functional health patterns for systematic nursing data collection based on Marjorie Gordon's framework.
Focuses on individual's health perception and behavior, including data on habits like smoking, and symptoms.
Examines food/fluid intake and potential health issues regarding metabolism and gastrointestinal systems.
Details the physical examination processes for assessing nutrition-related health parameters.
Focus on excretion patterns and issues like incontinence or constipation, including subjective/objective data collection.
Assesses daily activities requiring energy expenditure, self-care, exercise, and evaluations of physical capabilities.
Evaluates cognitive skills, sensory functions, and subjective experiences regarding memory and pain.
Focus on sleep patterns, relaxation strategies, and assessments for sleep-related issues.
Explores individuals' self-esteem, body image, and attitudes, measuring self-worth and personal experiences.
Looks at personal relationships, role satisfaction, and social interactions affecting health status.
Discusses reproductive health issues, satisfaction, and concerns regarding sexuality and related assessments.
Evaluates stress perception, coping strategies, and support systems to manage life's challenges.
Focuses on individual values, beliefs, and future plans, including the role of spirituality in decision-making.
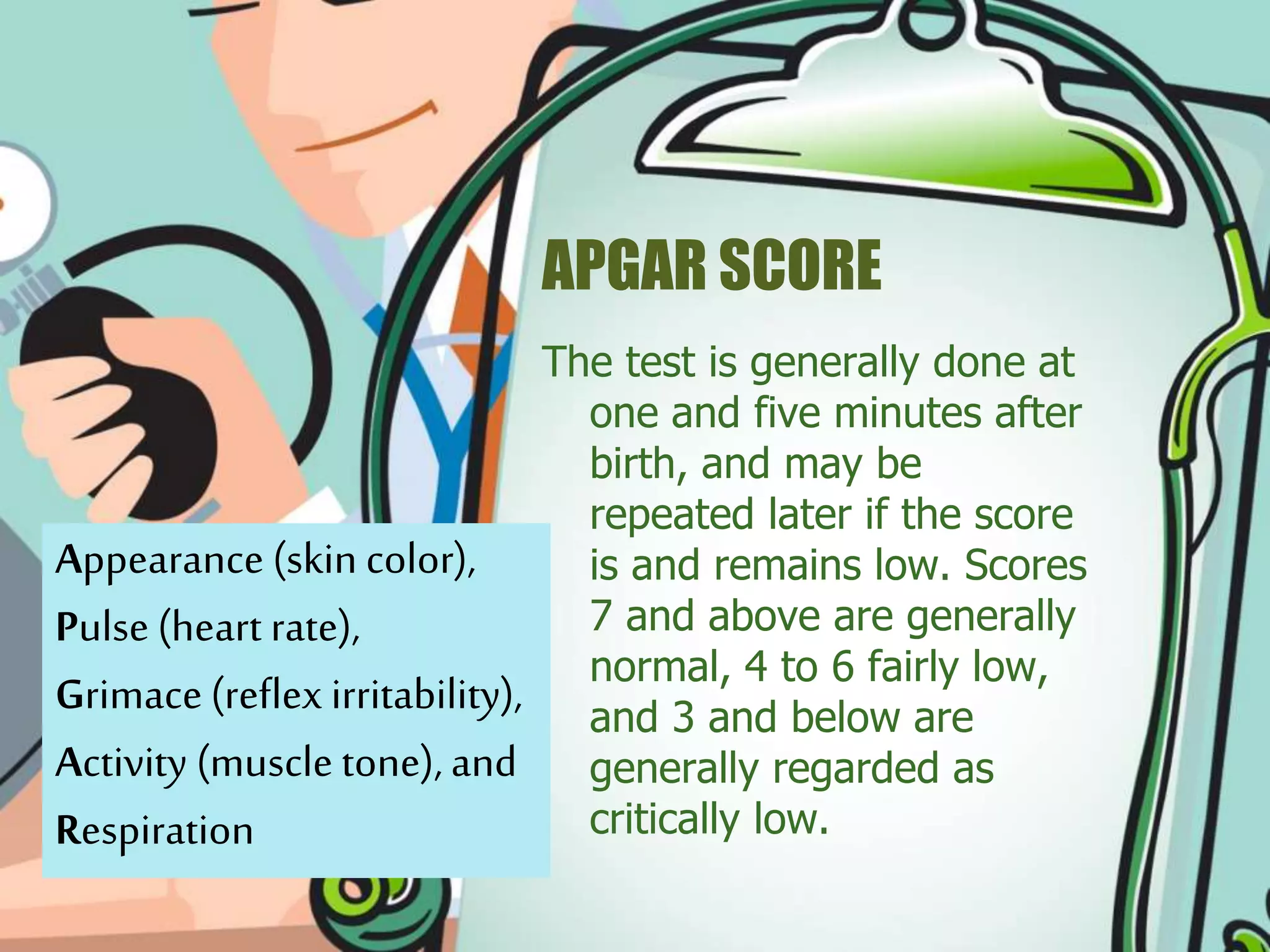
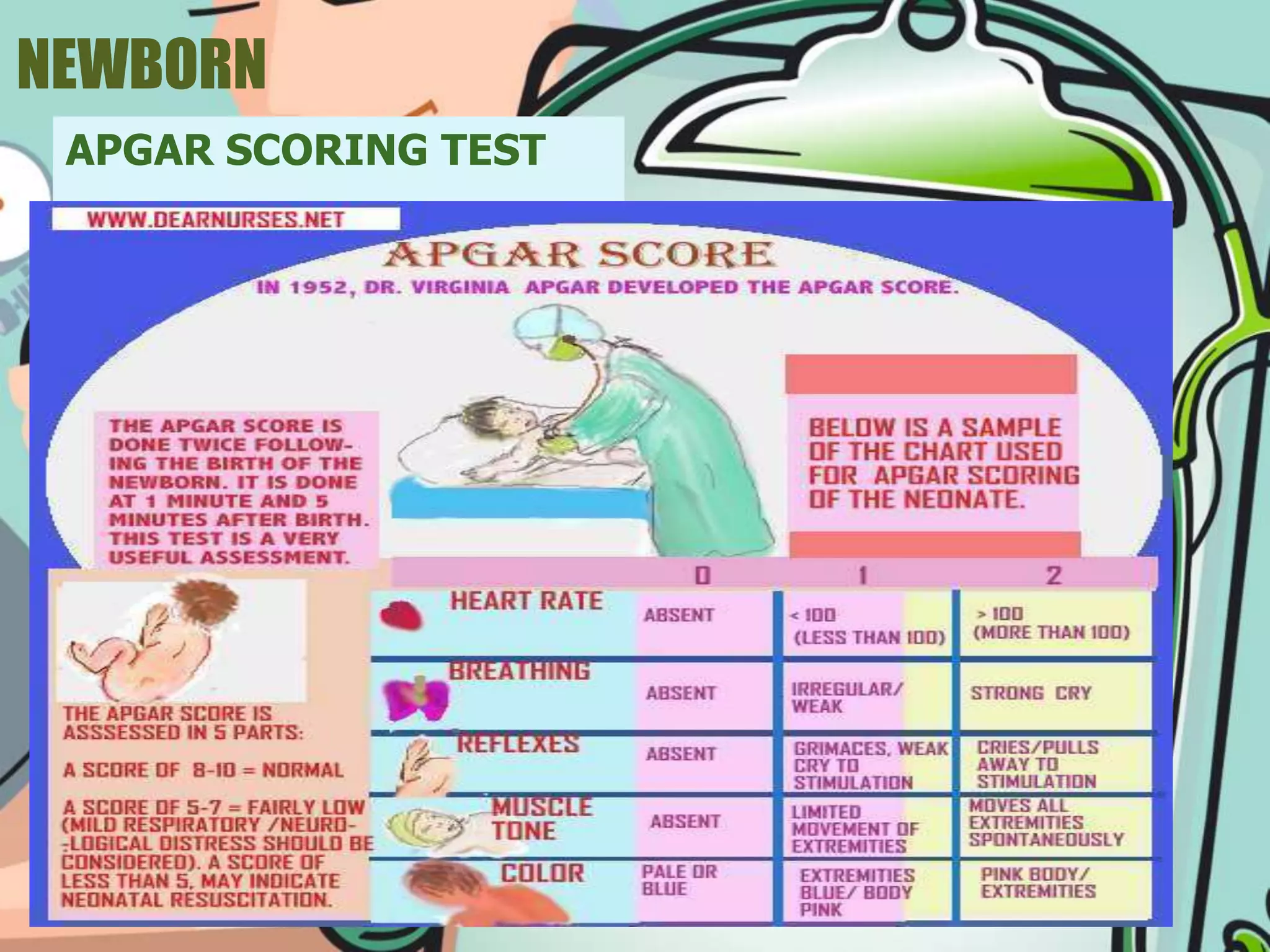
Introduces the APGAR score, a health assessment for newborns, detailing criteria and scoring norms.
Discusses newborn screening programs aimed at early identification of health issues and legislative background.
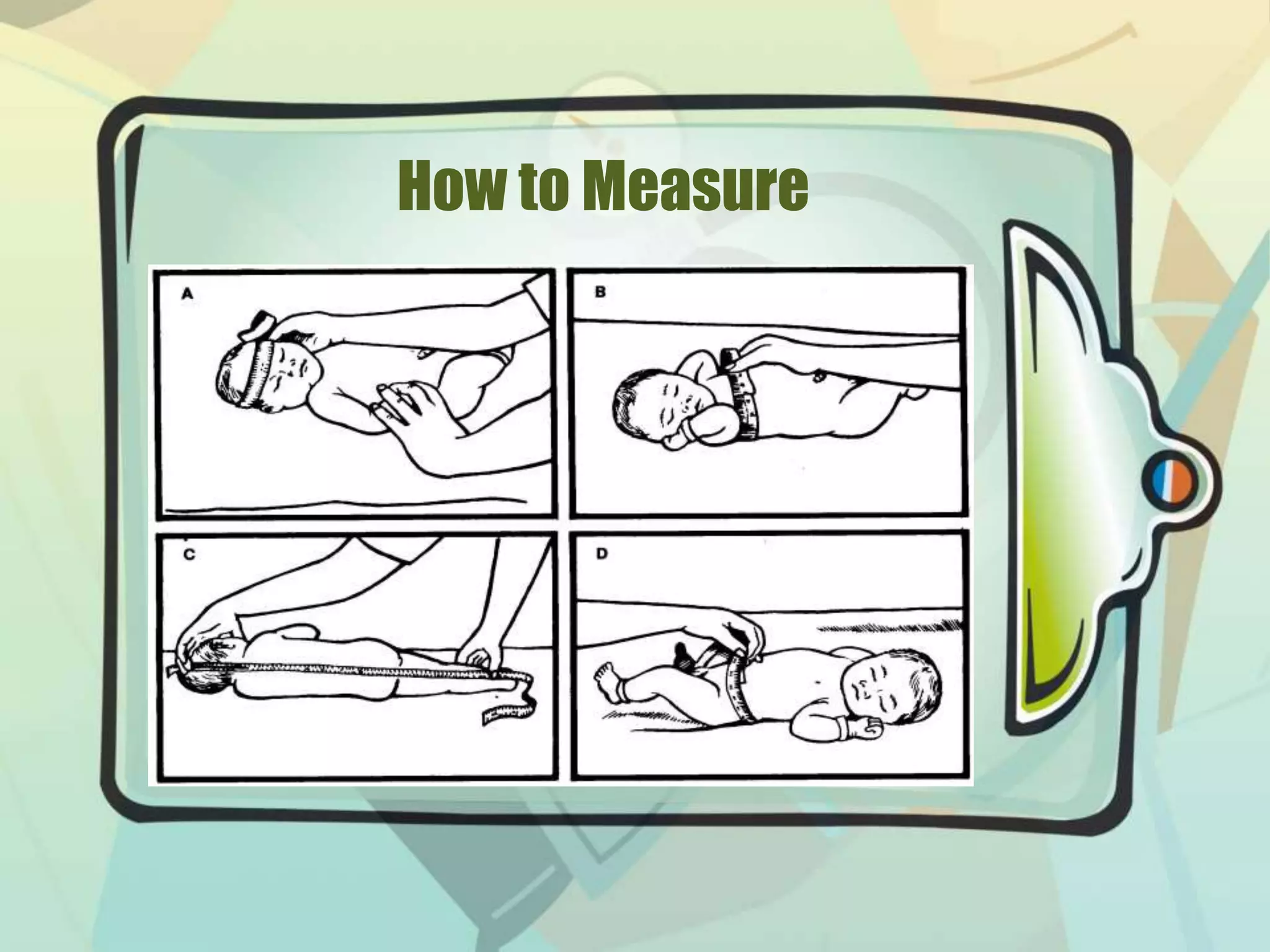
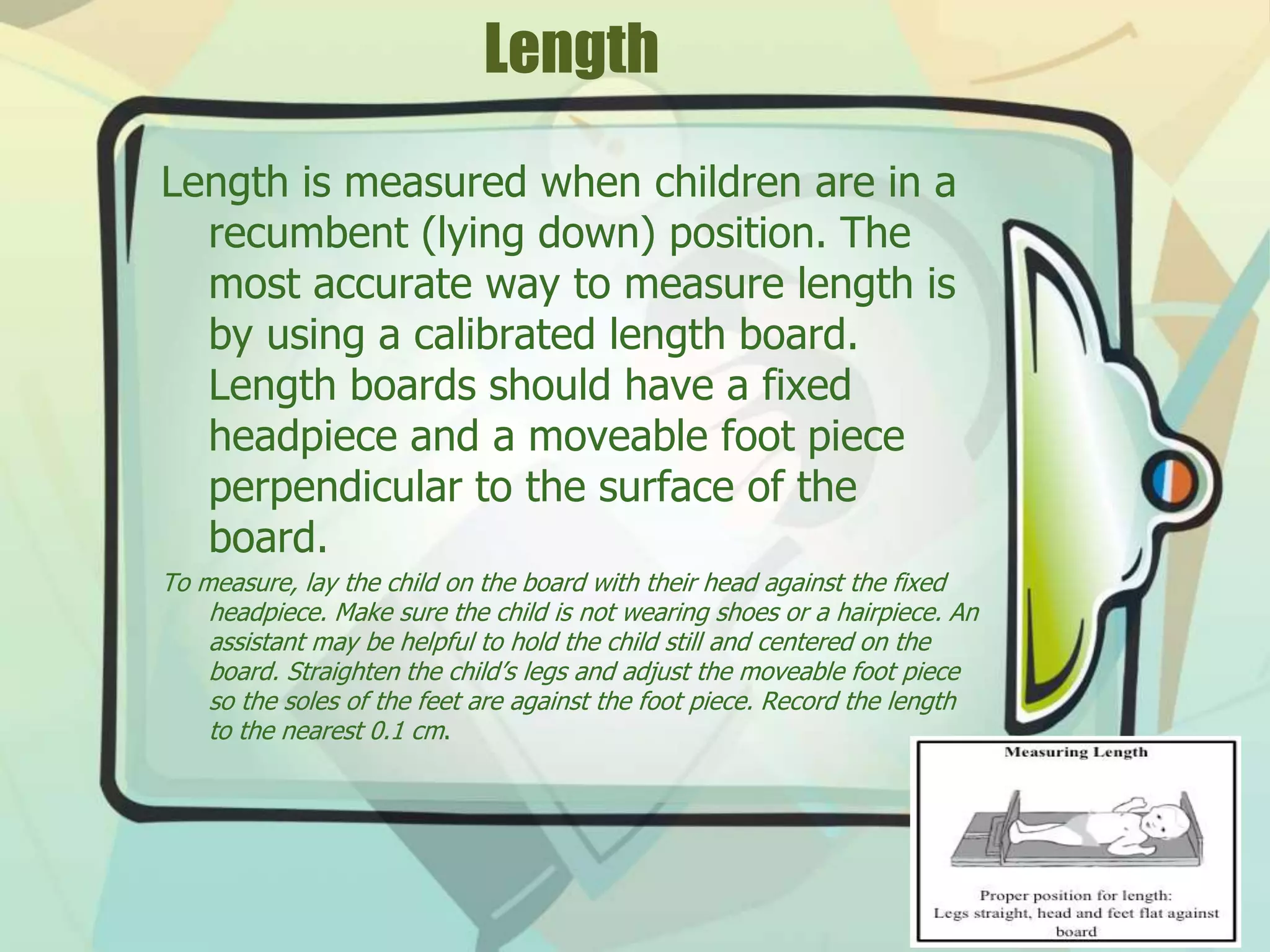
Explains the importance of measuring height, length, and weight for monitoring child growth and development.
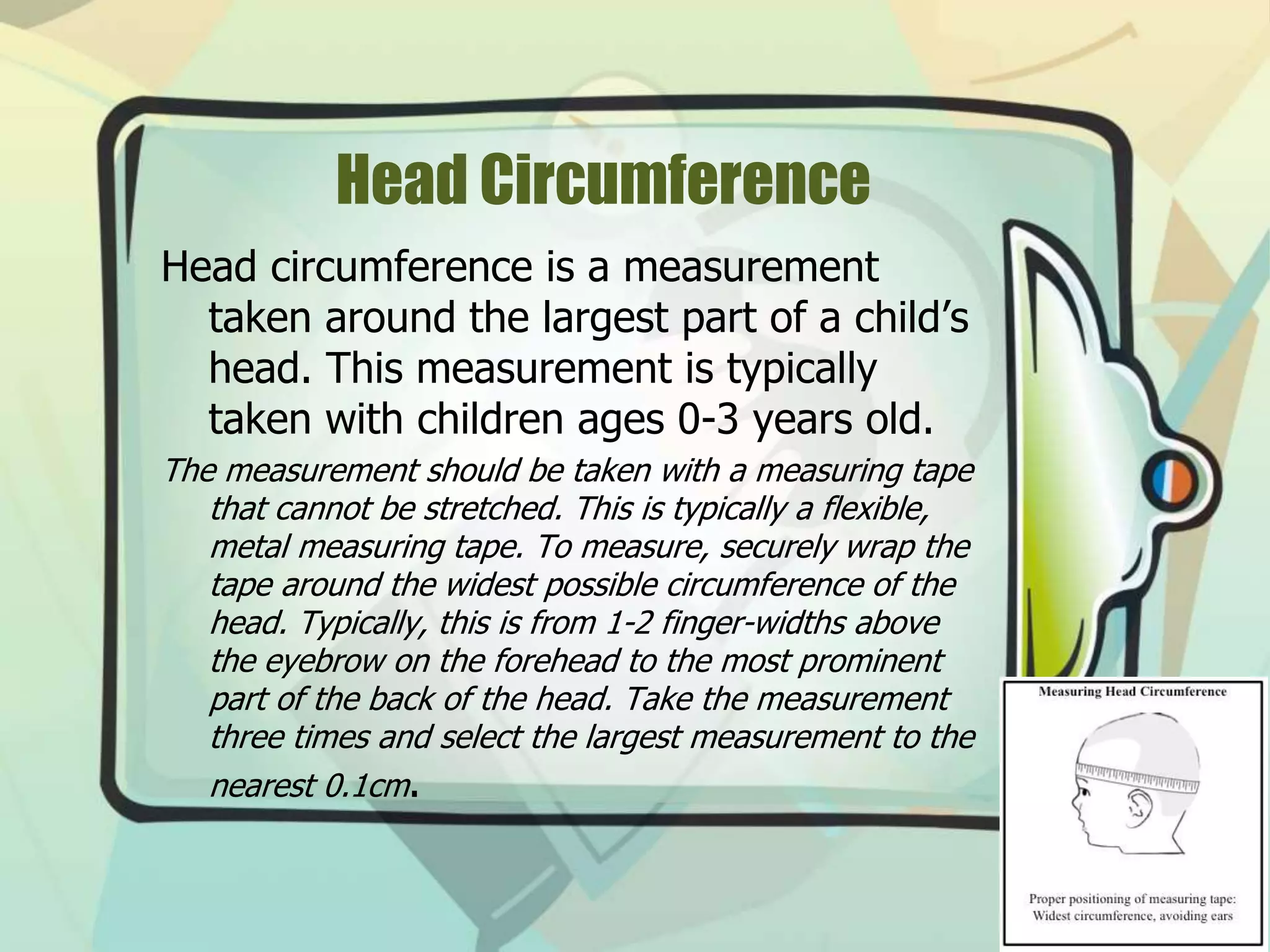
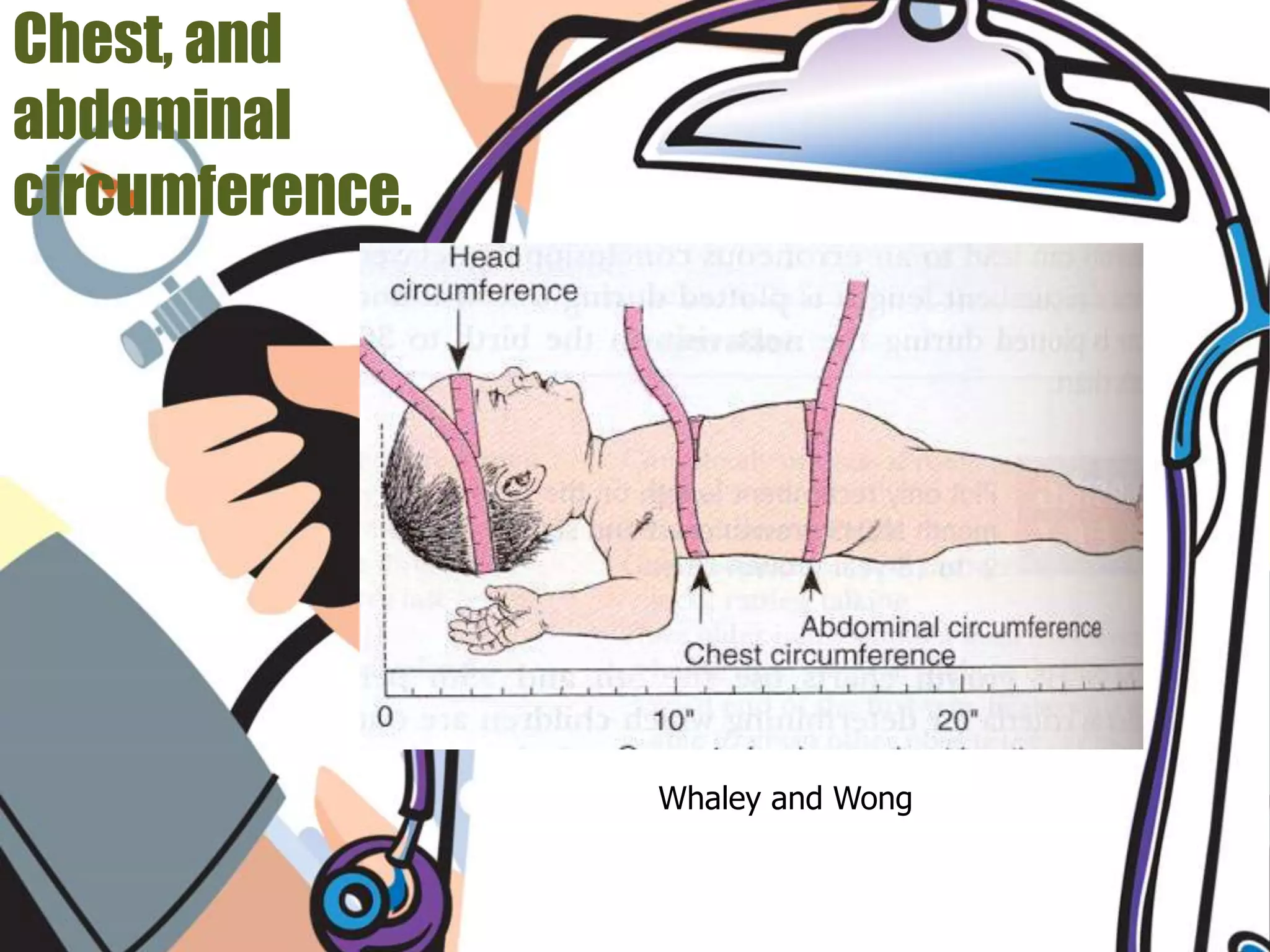
Describes procedures for accurately measuring head circumference and the significance of this measurement.
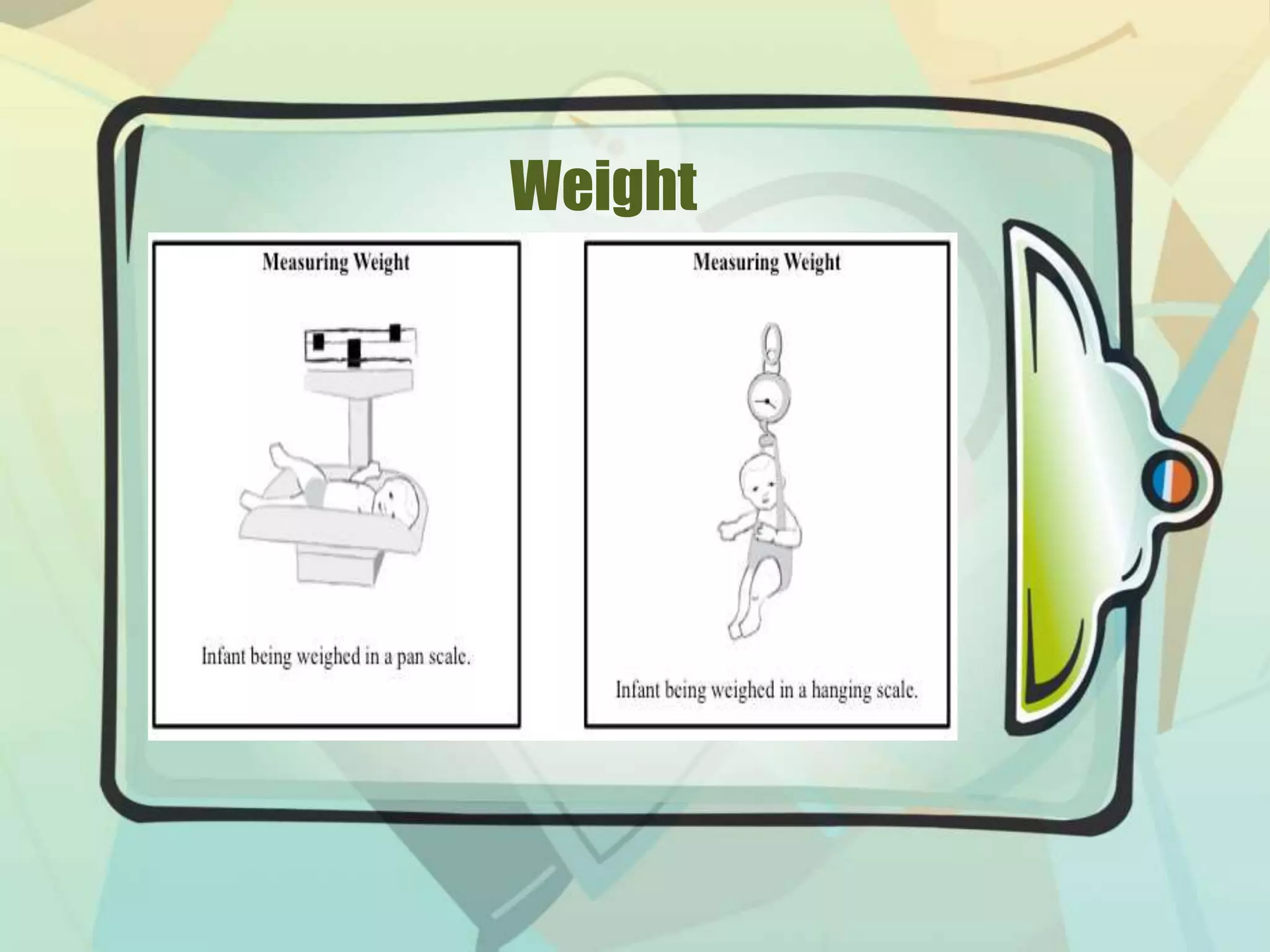
Details various methods of weighing infants and the importance of tracking weight as a health indicator.
Introduces the MMDST and Katz Index for assessing developmental delays and functional independence in adults.
Explains how to calculate BMI, its significance in health assessments, and categorizes weight status.