



























































![There are two processes in the production of speech
1] Phonation –it is the production of airflow and the
establishment of frequency
2] Articulation- it is the modification of airflow by
resonance or various degree of stoppage to produce
vowels and consonants
www.indiandentalacademy.com](https://image.slidesharecdn.com/functionalappliancespart-iphilosophyandvariousstudiesservosystemtheory-160425135523/75/Functional-appliances-philosophy-and-various-studies-servo-system-theory-193-2048.jpg)































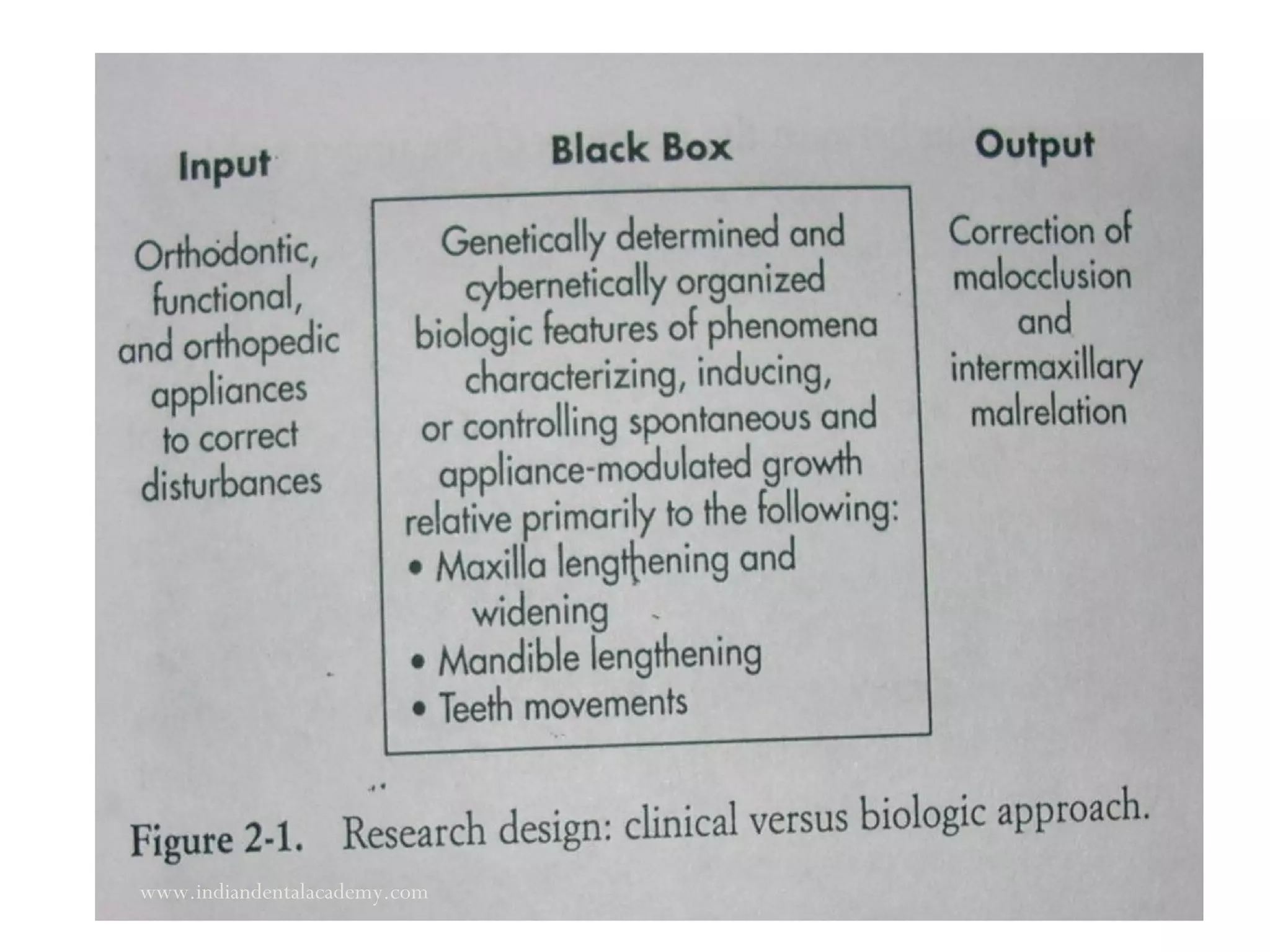
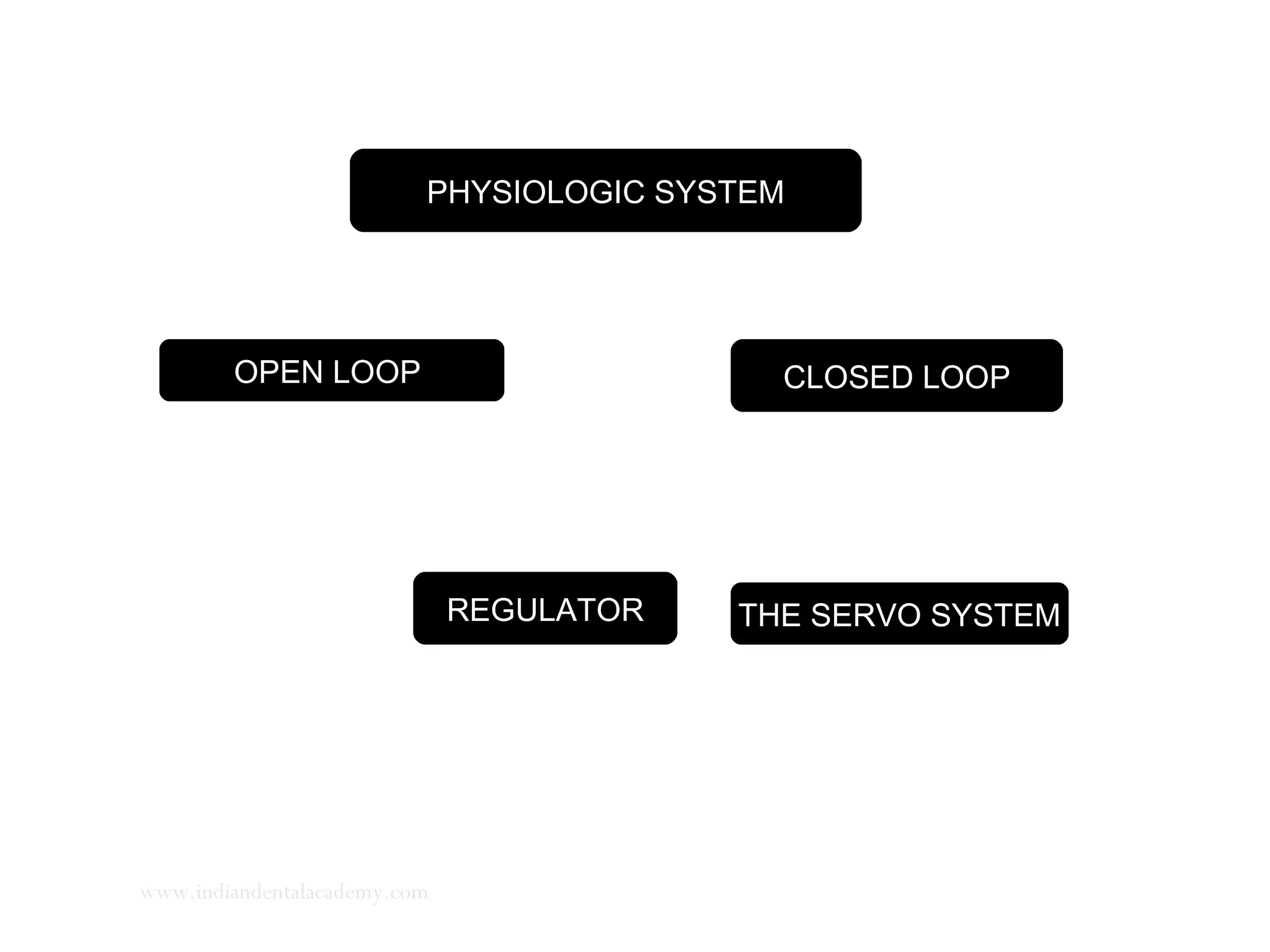
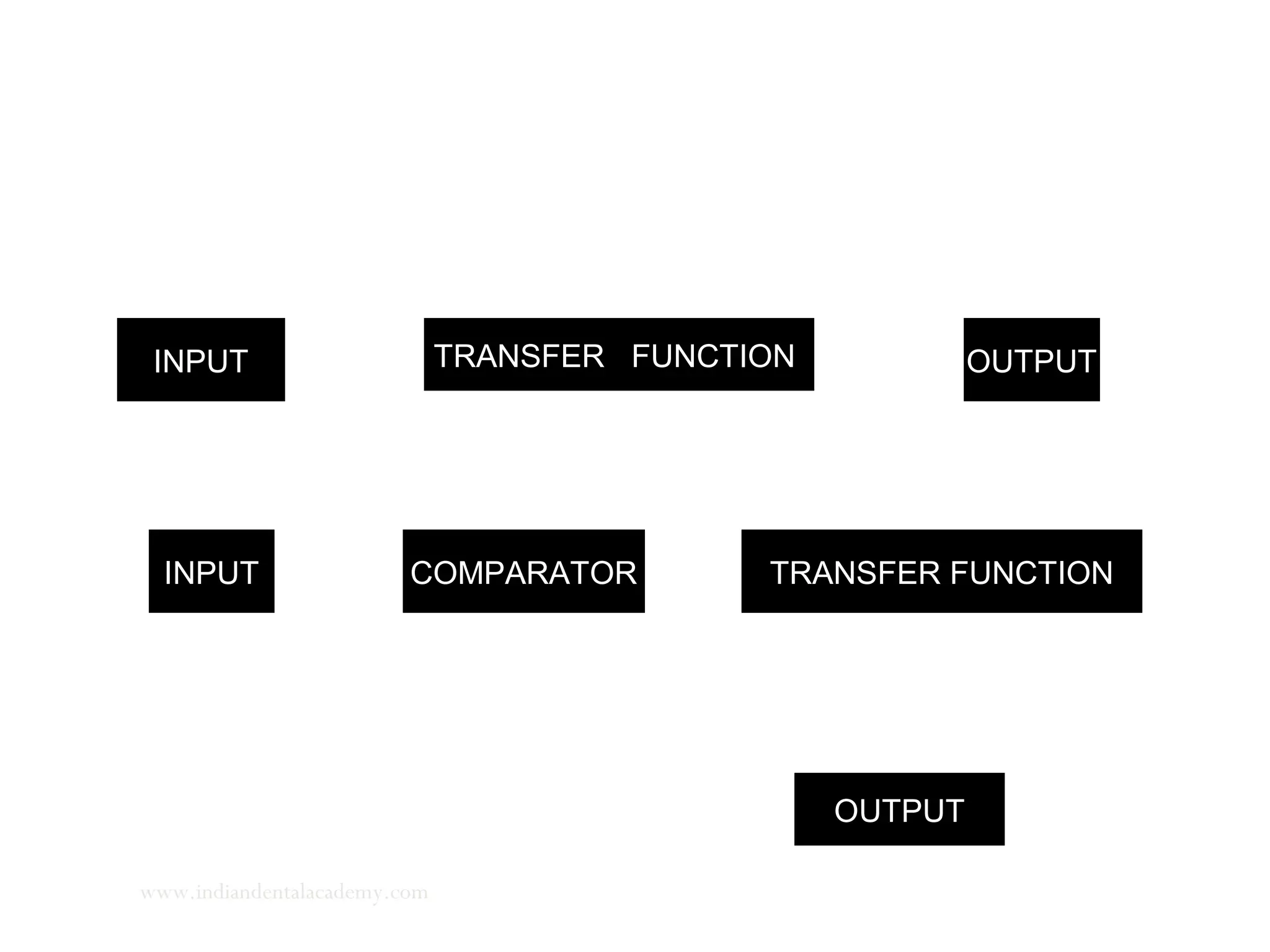
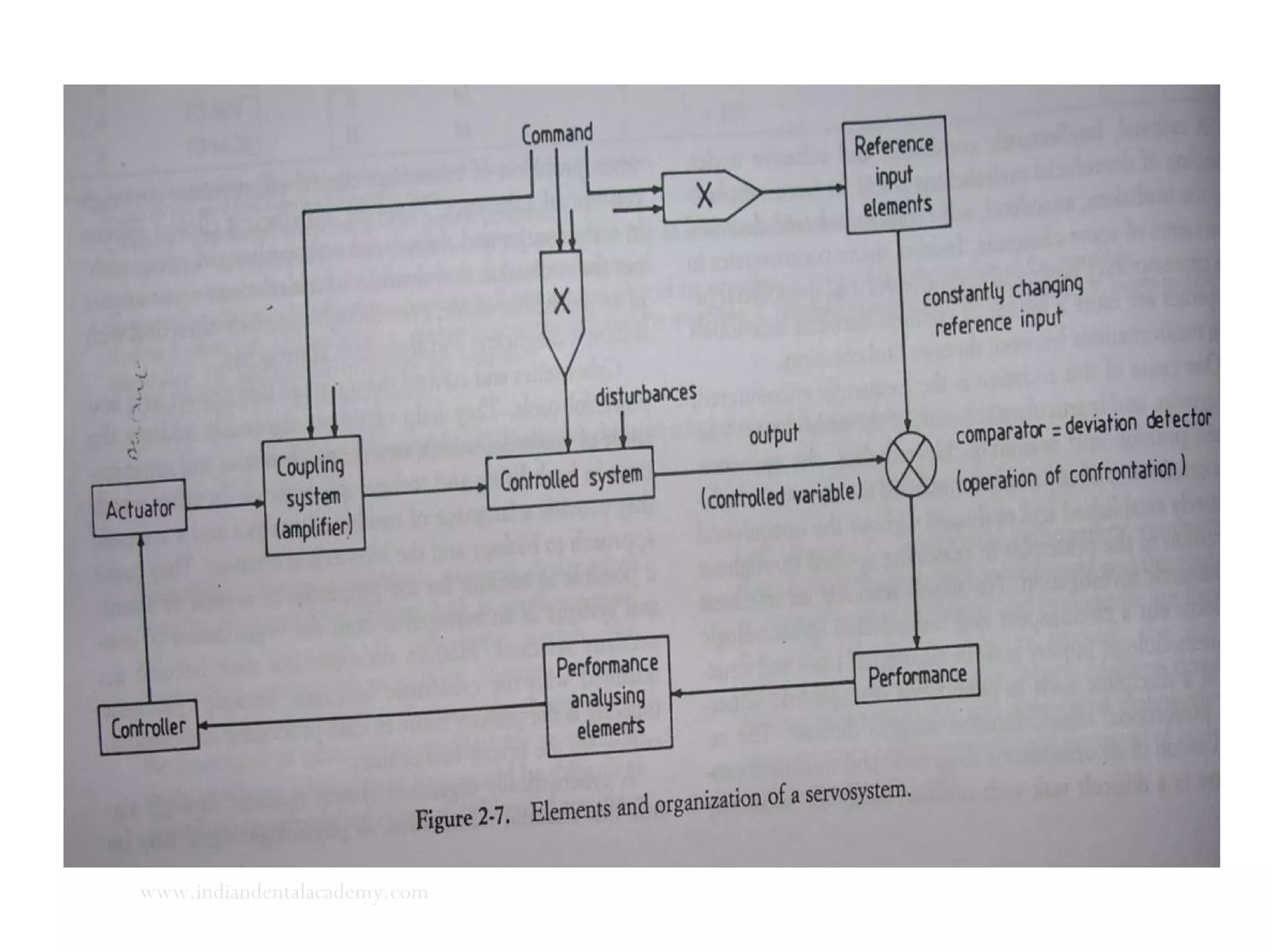
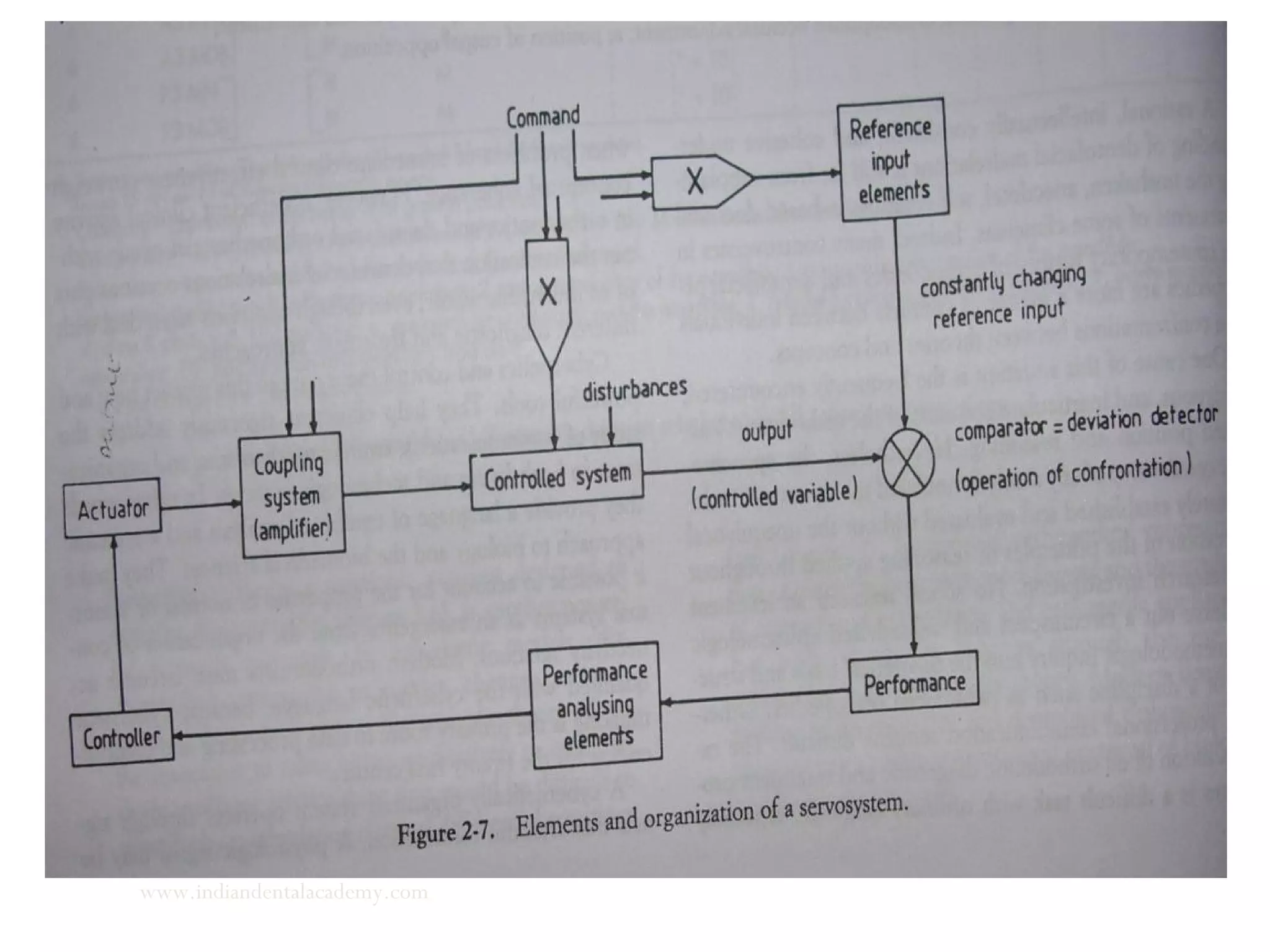
The document discusses the philosophy and functional applications of cybernetics in craniofacial growth, emphasizing how functional appliances can modify the growth of condylar cartilage and impact orthodontic practices. It outlines the components of servosystems, explaining how feedback mechanisms relate to the management and control of mandibular and maxillary growth. The integration of cybernetics into orthodontics enhances understanding of complex growth processes and the influences of hormonal and functional factors on bone development.





























































































