
![GOVERNMENT OF INDIA POLICY ON
TELEMEDICINE
EHR Standards notified. Available on
MoHFW website.
MDDS Standards draft approved.
Available on MoHFW website
Telemedicine Guidelines published.
Digital India > eKranti > eHealth
Services > Telemedicine
DEITY > NeGP > MMP > Health
National eHealth Authority [NeHA] in the
works.
8](https://image.slidesharecdn.com/frenchtelemed22jan15v2-150317094632-conversion-gate01/85/French-telemed-22-jan15-v2-8-320.jpg)
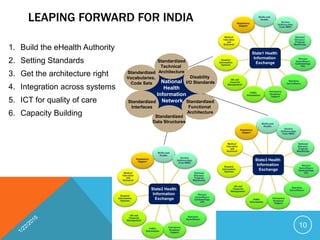
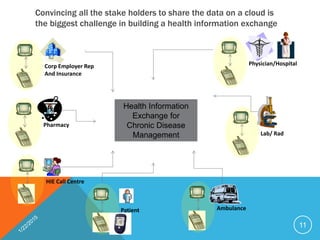


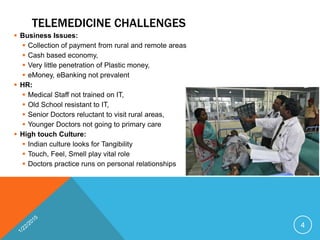
The document outlines the overview and potential of telemedicine in India, highlighting its various technologies and applications to address healthcare gaps in rural areas due to workforce shortages and accessibility issues. It discusses the challenges of implementing telemedicine, including payment collection in rural economies and resistance from medical staff. The document also includes government policies and initiatives aimed at enhancing telemedicine infrastructure and services.






















































































