

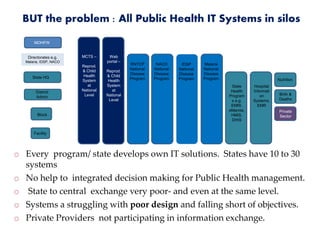
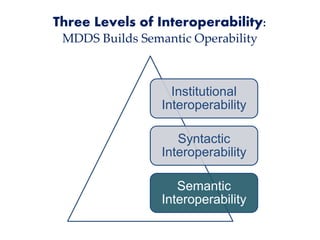
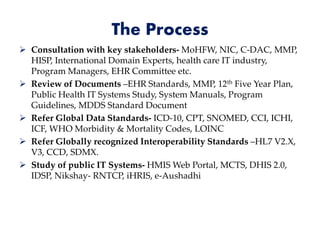
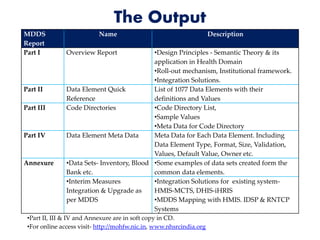
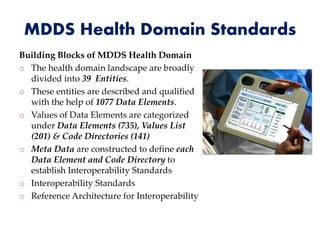
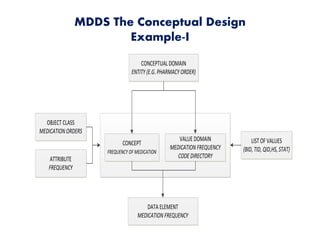
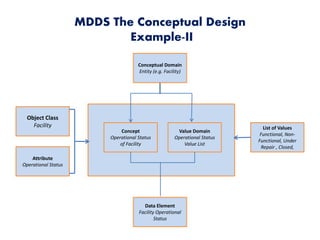
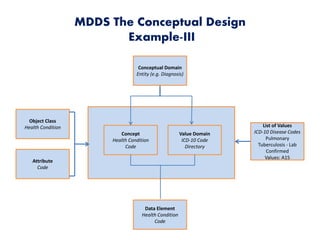
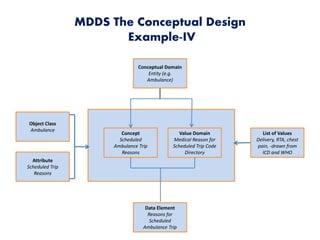
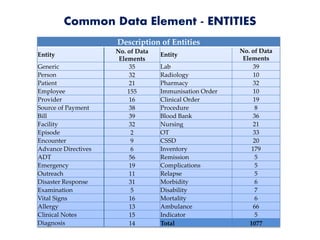
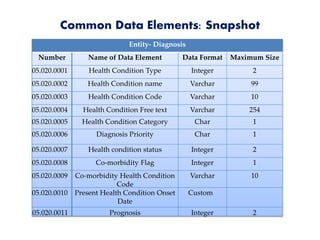
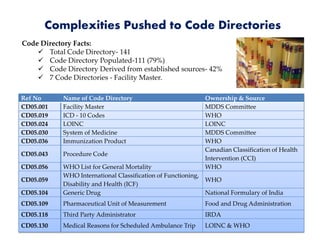
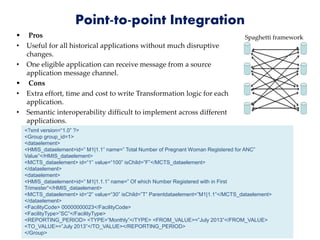


The document describes the development of metadata and data standards for the health domain in India by the Health MDDS Domain Committee. The committee was formed to promote interoperability across health IT systems. It identified over 1000 common data elements across 39 health entities. It defined the data elements and established 111 code directories derived from global clinical coding standards. The standards are intended to enable integration and information exchange between existing fragmented health IT systems in India.






































![Health delivery information system [HDIS] MVP](https://cdn.slidesharecdn.com/ss_thumbnails/healthdeliveryinformationsystemhdismvp-210419073440-thumbnail.jpg?width=640&height=640&fit=bounds)





























![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

















