Flexes, adducts and internally rotates the hip
Surgeon:
- Posterior approach:
- Identifies fracture site
- Reduces fracture under direct vision
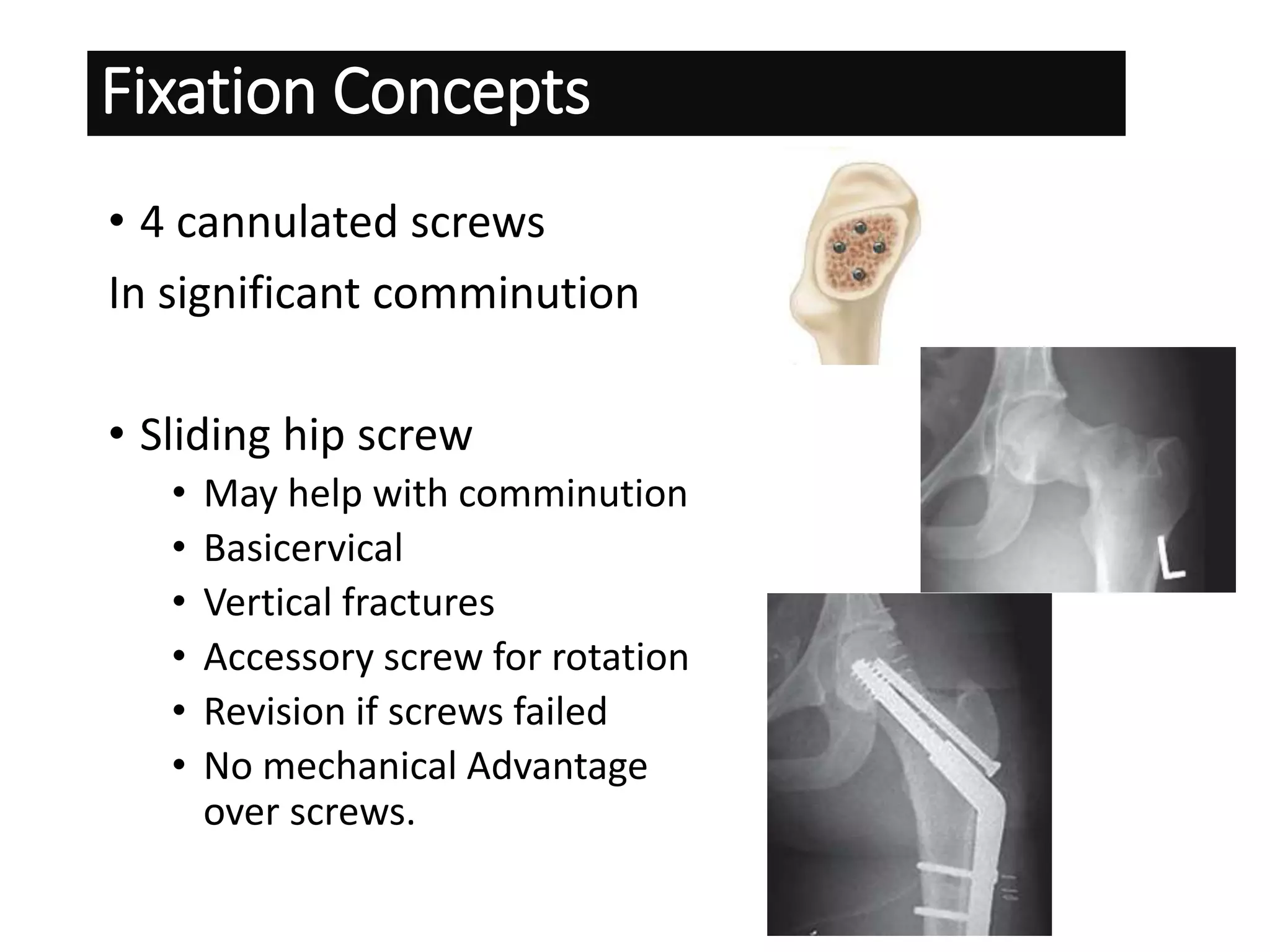
- Fixation with cannulated screws or sliding hip screw
- Capsulotomy allows decompression and reduction
- Closed suction drain
- Post-op hip in flexion, adduction, internal rotation
- Weight bearing as tolerated
- Follow up x-rays at 6 weeks, 3 months, 6 months
- Non-union, AVN, implant failure are complications
Open Reduction allows direct visualization and anatomic reduction