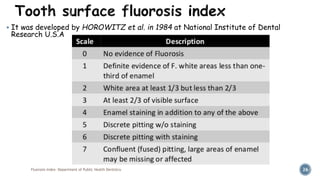
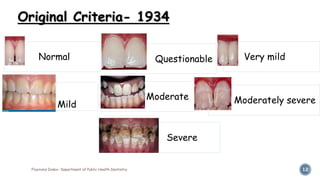
The document discusses dental fluorosis, its characteristics, and the indices used to assess its severity, including Dean's Fluorosis Index and the Thylstrup and Fejerskov Index. It highlights the effects of excessive fluoride ingestion during tooth development, describing various forms and classifications of fluorosis. Additionally, it elaborates on the examination methods and public health significance of measuring dental fluorosis in populations.



![ It attempts to validate the visual appearance against the histological defect.
Most sensitive of all fluorosis measuring indices.
Studies have concluded that the T-F index is the most indicated for work
where detailed information about the problem is required.
[Cleaton-Jones and Hargreaves (1990) ; Granath et al. (1985)]
Clarkson (1989) reported that in TF index drying of teeth creates an
unnatural situation due to which changes in score 1 and 2 are very minor.
The aesthetic significance of these changes are questionable.
Fluorosis Index- Department of Public Health Dentistry 25
Disadvanta
ges](https://image.slidesharecdn.com/fluorosisindex-161009154540/85/Fluorosis-index-25-320.jpg)