Downloaded 1,035 times
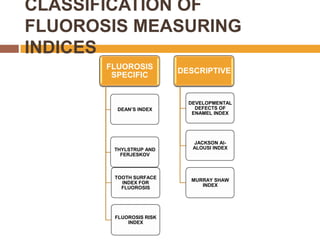
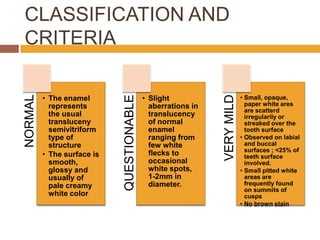
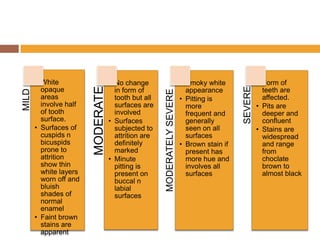
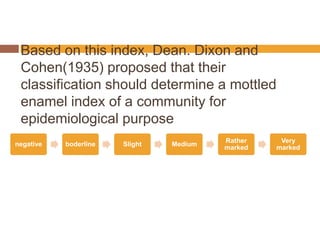

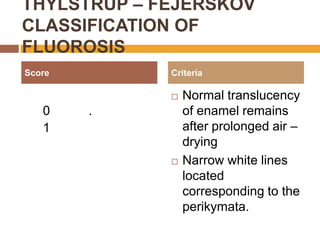
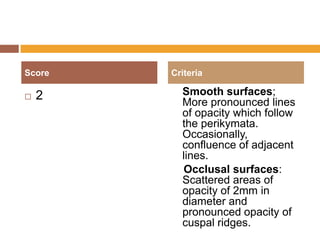
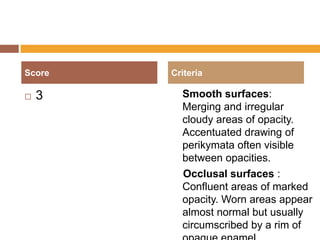
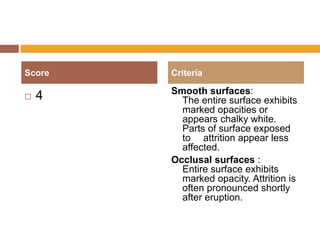

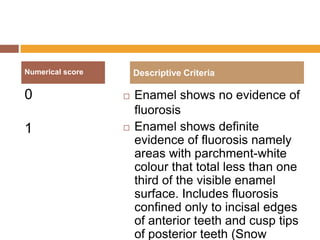
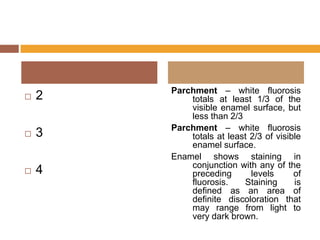
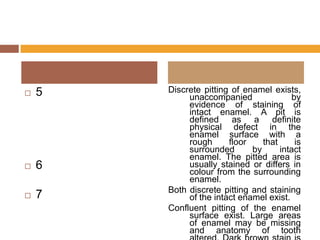
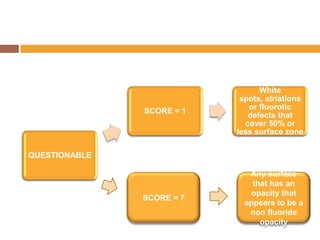
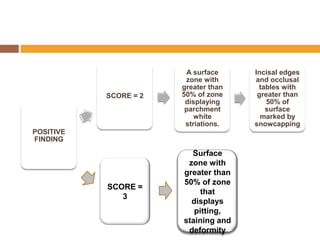

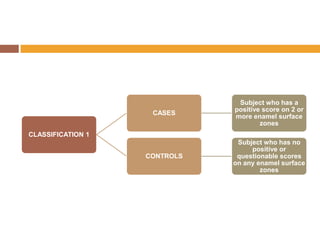
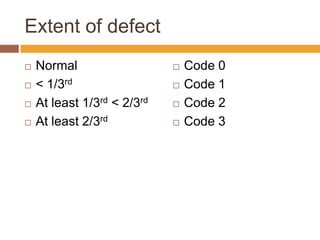
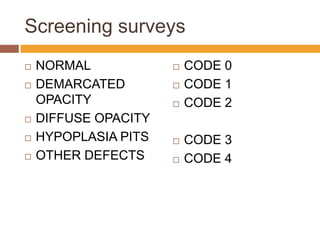
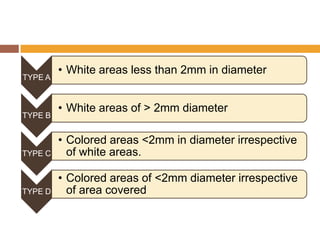
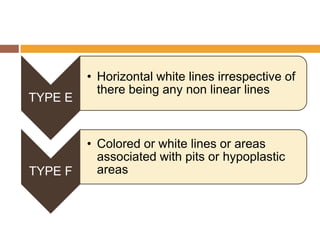
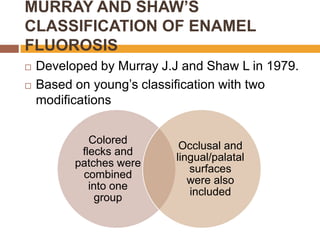

This document provides information on various indices used to measure dental fluorosis, including Dean's Index created in 1934, the Thylstrup-Fejerskov classification from 1978, and the Tooth Surface Fluorosis Index developed in 1984. It describes the classification criteria and scoring systems for each index, along with their uses, advantages, and limitations. Dean's Index is noted as the most widely used to measure dental fluorosis and helped indicate fluorosis prevalence in many communities. The Thylstrup-Fejerskov classification is described as the most sensitive index.























































































