













![Health Benefits of Work
• Good Work is Good for Health
• Focus on ‘Capacity’ not ‘Incapacity’ [Fit Note?]
• Early intervention is cost effective: Primary care,
workplaces, secondary care all play a part
• Work should be regarded as a clinical outcome of care
• Up to 30% of workers with MSDs also have mental
health problems – interventions need to take this into
account
• Work has therapeutic benefits – especially ‘good work’
– but what does this mean in practice?](https://image.slidesharecdn.com/fitforwork-140915224312-phpapp01/85/Fit-for-Work-16-320.jpg)









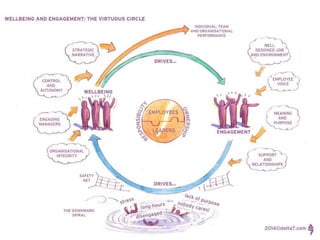










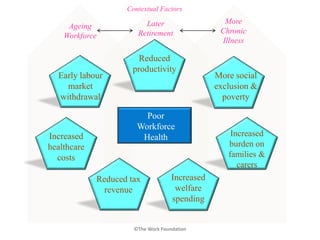
The document discusses the impact of musculoskeletal disorders (MSDs) on the workforce, highlighting their significant burden as a leading cause of disability globally. It emphasizes the importance of early intervention and the promotion of 'good work' to enhance employee health, engagement, and productivity, particularly in the face of an ageing workforce. Strategies for improving workplace well-being are outlined, focusing on prevention, support systems, and the economic benefits of maintaining a healthy workforce.



















































































