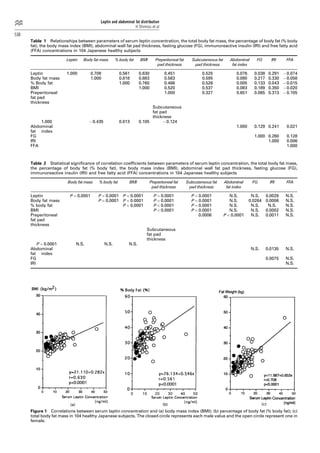
This study investigates the relationship between serum leptin concentrations and body fat parameters in 104 healthy Japanese subjects. Results show that serum leptin is significantly correlated with total body fat mass, body fat percentage, and BMI, but not with abdominal fat distribution. A four-week food restriction reduced both serum leptin levels and body fat mass, although the percentage change in leptin did not correlate with the change in body fat.












![우리 뇌는 식욕을 어떻게 조절할까? [2016 대한청소년정신의학회 추계학술대회]](https://cdn.slidesharecdn.com/ss_thumbnails/20161013-170201014103-thumbnail.jpg?width=640&height=640&fit=bounds)








![뇌와 비만 - 신경과 지방, 간, 췌장, 위장관 연결 [2016년 대한비만학회 연수강좌]](https://cdn.slidesharecdn.com/ss_thumbnails/20160221-170201014907-thumbnail.jpg?width=640&height=640&fit=bounds)
































![Guidelines heart rate_variability_ft_1996[1]](https://cdn.slidesharecdn.com/ss_thumbnails/guidelinesheartratevariabilityft19961-100604162052-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Pulseox[1]](https://cdn.slidesharecdn.com/ss_thumbnails/pulseox1-100604162535-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)




































