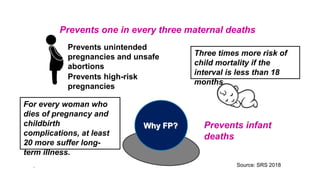
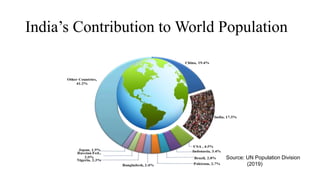
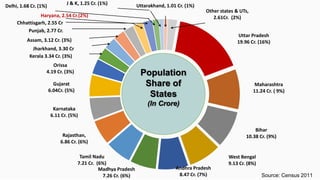
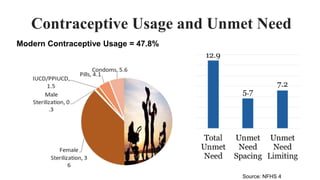
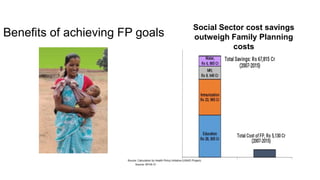
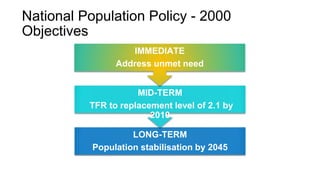
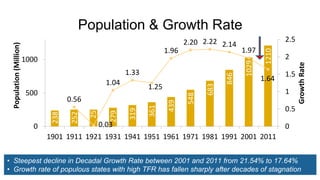
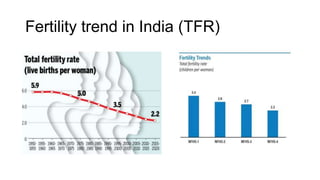
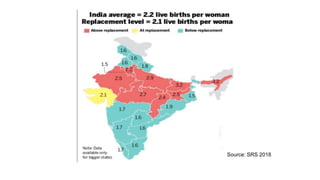
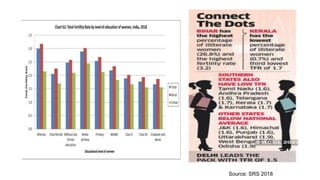
The document outlines the importance of family planning in India, emphasizing its role in preventing maternal and infant mortality, addressing unmet contraceptive needs, and stabilizing population growth. It discusses various family planning methods, including both temporary and permanent options, and highlights the National Family Planning Program and its key initiatives aimed at improving access to family planning services. Additionally, it details demographic statistics and trends in contraceptive usage, as well as challenges and objectives associated with family planning in the country.






































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)













