Download to read offline

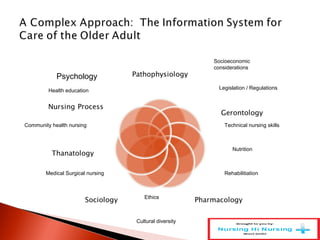






This document discusses parish nursing and its role in caring for older adults within faith communities. It begins by defining parish nursing as a specialty practice that combines nursing and health ministry, rooted in Judeo-Christian traditions. It describes how parish nurses collaborate with pastoral staff and congregants to promote health and healing. They partner with other health resources to create new responses to health concerns. The document emphasizes that parish nurses serve communities with compassion, advocating for individuals with dignity. It highlights opportunities for parish nurses to address older adults' diverse needs through a variety of nursing specialties and approaches.