Facilitating Cognitive Assessment in Primary Care for the Timely Detection of Alzheimer’s Disease: Leveraging Medicare Reimbursement Mechanisms to Improve Clinical Care
•
0 likes•17 views

Co-Chairs, Anna Chodos, MD, MPH, and Ian Neel, MD, prepared useful Practice Aids pertaining to Alzheimer’s disease for this CME/MOC/NCPD/CPE/APA/IPCE activity titled “Facilitating Cognitive Assessment in Primary Care for the Timely Detection of Alzheimer’s Disease: Leveraging Medicare Reimbursement Mechanisms to Improve Clinical Care.” For the full presentation, downloadable Practice Aids, and complete CME/MOC/NCPD/CPE/APA/IPCE information, and to apply for credit, please visit us at https://bit.ly/3htC9KO. CME/MOC/NCPD/CPE/APA/IPCE credit will be available until May 25, 2024.

Recommended
Recommended
More Related Content
Similar to Facilitating Cognitive Assessment in Primary Care for the Timely Detection of Alzheimer’s Disease: Leveraging Medicare Reimbursement Mechanisms to Improve Clinical Care
Similar to Facilitating Cognitive Assessment in Primary Care for the Timely Detection of Alzheimer’s Disease: Leveraging Medicare Reimbursement Mechanisms to Improve Clinical Care (20)
More from PVI, PeerView Institute for Medical Education
More from PVI, PeerView Institute for Medical Education (20)
Recently uploaded
Recently uploaded (20)
Facilitating Cognitive Assessment in Primary Care for the Timely Detection of Alzheimer’s Disease: Leveraging Medicare Reimbursement Mechanisms to Improve Clinical Care
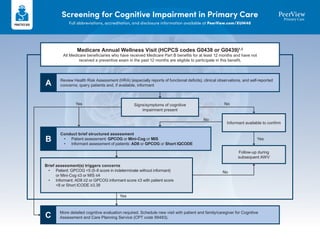
- 1. Screening for Cognitive Impairment in Primary Care Full abbreviations, accreditation, and disclosure information available at PeerView.com/XUM40 Medicare Annual Wellness Visit (HCPCS codes G0438 or G0439)1,2 All Medicare beneficiaries who have received Medicare Part B benefits for at least 12 months and have not received a preventive exam in the past 12 months are eligible to participate in this benefit. Review Health Risk Assessment (HRA) (especially reports of functional deficits), clinical observations, and self-reported concerns; query patients and, if available, informant A Conduct brief structured assessment • Patient assessment: GPCOG or Mini-Cog or MIS • Informant assessment of patients: AD8 or GPCOG or Short IQCODE B More detailed cognitive evaluation required. Schedule new visit with patient and family/caregiver for Cognitive Assessment and Care Planning Service (CPT code 99483). C Signs/symptoms of cognitive impairment present Informant available to confirm Follow-up during subsequent AWV Brief assessment(s) triggers concerns • Patient: GPCOG <5 (5-8 score in indeterminate without informant) or Mini-Cog ≤3 or MIS ≤4 • Informant: AD8 ≥2 or GPCOG informant score ≤3 with patient score <8 or Short ICODE ≥3.38 Yes Yes Yes No No No
- 2. Screening for Cognitive Impairment in Primary Care Full abbreviations, accreditation, and disclosure information available at PeerView.com/XUM40 A • Review and update medical and family history • Review and update list of current providers • Measure height, weight, BMI, blood pressure • Review potential risk factors for depression or other mood disorders (first AWV only) • Review functional ability and level of safety (first AWV only) • Establish or update screening schedule for next 5-10 years • Prepare list of risk factors and conditions for which interventions are recommended, and a list of treatment options and their associated risks and benefits • Provide health advice and referral, as appropriate, to health education or preventive counseling services or programs, designed to reduce risk factors, such as for weight loss, smoking cessation, fall prevention, and nutrition • Assess for any signs of cognitive impairment: ✓ Any red flags in the HRA? ✓ Observations by clinicians (medical and associated staff)? ✓ Acknowledgment of any self-reported or informant-reported concerns? ✓ Conversational queries about cognition directed toward the patient and others present, such as: ❑ During the past 12 months, have you experienced confusion or memory loss that is happening more often or is getting worse? ❑ During the past 7 days, did you need help with others to perform everyday activities such as eating, getting dressed, grooming, bathing, walking, or using the toilet? ❑ During the past 7 days, did you need help from others to take care of things such as laundry and housekeeping, banking, shopping, using the telephone, food preparation, transportation, or taking your own medications? Review Health Risk Assessment1,2 If signs/symptoms of cognitive impairment are present, go to B
- 3. Screening for Cognitive Impairment in Primary Care Full abbreviations, accreditation, and disclosure information available at PeerView.com/XUM40 1. Cordell CB et al. Alzheimers Dement. 2013;9:141-150. 2. https://www.alz.org/media/Documents/factsheet-medicare-annual-wellness-visit-2017.pdf. 3. Galvin JE et al. Neurology. 2005;65:559-564. 4. Brodaty H et al. Int J Geriatr Psychiatry. 2004;19:870-874. 5. Buschke H et al. Neurology. 1999;52:231-238. 6. Borson S et al. Int J Geriatr Psychiatry. 2000;15:1021-1027. 7. https://knightadrc.wustl.edu/professionals-clinicians/ad8-instrument/. 8. https://gpcog.com.au/. 9. https://www.alz.org/media/documents/memory-impairment- screening-mis.pdf. 10. https://mini-cog.com/download-the-mini-cog-instrument/. Tool Brief Description Scoring and Interpretation Informant-Based Assessments Ascertain Dementia 8-Item Informant Questionnaire (AD8)7 https://knightadrc.wustl.edu/ professionals-clinicians/ad8- instrument/ • Brief informant-based questionnaire • 8 yes/no questions designed to assess changes in the past few years in memory, orientation, executive functioning and/or interest in activities • Approximately 3 min to complete • Scores based upon number of ‘yes’ answers – Range from 0 to 8 – Normal: 0-1 – Cognitive impairment likely: ≥2 GPCOG Informant8 https://gpcog.com.au/ • Screening tool designed for GPs, PCPs, FMs • Takes 2 minutes to complete informant interview • Informant is asked about the patient’s memory of recent conversations, misplacing objects, word finding difficulties, ability to manage money, ability to manage medication, and need for travel assistance • Informant interview should be administered if GPCOG-patient score lies between 5 and 8 • GPCOG-informant maximum score = 6 • GPCOG-informant score of 3 or lower suggests cognitive impairment Patient-Based Assessments GPCOG Patient8 https://gpcog.com.au/ • Takes 4 minutes to administer patient assessment • Contains the following cognitive test items: time orientation, clock drawing, reporting a recent event, word recall task • GPCOG-patient maximum score of 9 indicates no cognitive impairment • If the GPCOG-patient score lies between 5 and 8 the GPCOG-informant should be administered • GPCOG-patient score of 4 or lower suggests cognitive impairment Memory Impairment Screen (MIS)9 https://www.alz.org/media/ documents/ memory-impairment- screening-mis.pdf • 4-item delayed free- and cued-recall test of memory impairment • Approximately 4 min to complete (plus a delayed recall section requiring delay of 5 min) • Score based upon recalling each word 5 min later; 2 points for spontaneous recall and 1 point for cued recall – Range from 0 to 8 – MCI: ≤5 – Dementia: ≤4 Mini-Cog10 https://mini-cog.com/ download-the-mini-cog- instrument/ • 2 components: 3-item recall test for memory and a simply scored clock drawing test • Approximately 3 min to complete • 5 total points possible; 1 point for each word remembered; and 2 points for a correctly drawn clock • Lower likelihood of dementia with total score of 3-5 B C Perform brief cognitive screening assessment (select one patient assessment and one informant assessment)1,3-6 If patient’s screen is positive, conduct a more detailed cognitive evaluation and development of a care plan (eg, CPT 99483)
- 4. Performing a Cognitive Assessment and Developing a Care Plan in Primary Care1-4 Full abbreviations, accreditation, and disclosure information available at PeerView.com/XUM40 Cognitive Assessment and Care Planning Services (CACP) CPT 99483 CACP services are provided when a comprehensive evaluation of a new or existing patient who exhibits signs and/or symptoms of cognitive impairment is required to establish or confirm a diagnosis, etiology, and severity for the condition. The following components are required for CPT code 99483 CACP Element Evaluation Points 1 Cognition-focused evaluation • Cognition-focused history and physical examination • Testing (eg, MMSE, MoCA, SLUMS, clock, GDS, cognitive domain deficits [memory, orientation, language, visuospatial, executive]) 2 Medical decision-making • Document medical decision-making of moderate or high complexity as defined by E/M guidelines 3 Functional assessment • Patient-reported preserved activities of daily living (ADLs), including advanced and instrumental ADLs • Caregiver-reported preserved ADLs, including advanced and instrumental ADLs • Executive decisional capacity 4 Dementia staging • Use standardized instruments for staging of dementia like the Functional Assessment Staging Test (FAST) and Clinical Dementia Rating (CDR) 5 Medication review • Medication reconciliation (including OTCs) • Determine any anticholinergics or sedative hypnotics • Determine who manages the patient’s medications and how 6 Neuropsychiatric/ behavioral evaluation • Use standardized screening instruments to evaluate for neuropsychiatric and behavioral symptoms, including depression and anxiety 7 Home safety evaluation • Conduct a safety evaluation (eg, driving, weapons, home, falls, medications) 8 Caregiver identification • Identify social supports including how much caregivers know and are willing to provide care 9 Advance care planning • Current advance directives (eg, DNR, POST/POLST, living will, POA), any palliative care needs 10 Written care plan • See page 5 for a helpful checklist Standardized assessment tools for the CACP can be downloaded from the following resources: Alzheimer’s Project Clinical Roundtable. Physician Guidelines for the Screening, Evaluation, and Management of Alzheimer’s Disease and Related Dementias: https://Championsforhealth.Org/Wp-content/Uploads/2021/09/Alzheimers-project-booklet-v11-082221-web.pdf Alzheimer’s Association. Cognitive Impairment and Care Planning Toolkit: https://www.alz.org/media/Documents/cognitive-impairment-care-planning-toolkit.pdf Page 1
- 5. Performing a Cognitive Assessment and Developing a Care Plan in Primary Care1-4 Full abbreviations, accreditation, and disclosure information available at PeerView.com/XUM40 COGNITIVE IMPAIRMENT VISIT TEMPLATE Patient name: DOB: CACP_1: Cognition-focused evaluation (reported from patient and caregiver) Cognitive history (patient): Cognitive history (informant): Testing MMSE: /30 (prior /30) MoCA: /30 (prior /30) SLUMS: /30 (prior /30) Clock: /3 GDS: /15 (prior /15) CACP_2: Discussion and Medical Decision Making (circle one) Low complexity | moderate complexity | high complexity CACP_3: Functional Assessment Reported from patient: Impaired instrumental activities of daily living (IADLs) (circle all that apply): Telephone | shopping | food prep | housekeeping | laundry | transportation | meds | finances Other: Impaired activities of daily living (ADLs) (circle all that apply): Bathing | toileting | grooming | feeding | transferring | continence Other: Reported from caregiver: Impaired instrumental activities of daily living (IADLs) (circle all that apply): Telephone | shopping | food prep | housekeeping | laundry | transportation | meds | finances Other: Impaired activities of daily living (ADLs) (circle all that apply): Bathing | toileting | grooming | feeding | transferring | continence Other: Assessment of patient’s decisional capacity (medical): | Yes | No | Uncertain Comment: Assessment of patient’s decisional capacity (executive): | Yes | No | Uncertain Comment: Cognitive domain deficits (circle one): • Memory: | Yes | No • Orientation: | Yes | No • Language: | Yes | No • Visuospatial: | Yes | No • Executive: | Yes | No Page 2
- 6. Performing a Cognitive Assessment and Developing a Care Plan in Primary Care1-4 Full abbreviations, accreditation, and disclosure information available at PeerView.com/XUM40 COGNITIVE IMPAIRMENT VISIT TEMPLATE CACP_4: Clinical dementia rating (severity): CACP_5: Medication Reconciliation (including OTCs) Anticholinergics/sedative hypnotics: | Yes | No Who manages the medications (patient or other) and how? CACP_6: Neuropsychiatric syndromes (behaviors, psychosis, depression, anxiety) and specifics: CACP_7: Safety concerns (driving, weapons, home, falls, medications, etc.) and specifics: CACP_8: Caregiver needs and current supports (respite, financial, education, etc.) and specifics: CACP_9: Current advance directives (DNR, POST/POLST, living will, POA, etc.) and specifics: Risk Factors (circle the correct responses below) Diabetes: | Yes | No Dyslipidemia: | Yes | No Hypertension: | Yes | No History of head injury with loss of consciousness: | Yes | No Sleep quality: | Yes | No Alcohol intake: | Yes | No Vision impairment: | Yes | No Hearing impairment: | Yes | No Depression: | Yes | No Page 3 Labs (circle all that apply) TSH | B12/Folate | CBC | CMP | Albumin/total protein | HIV | RPR Other: Radiology Head imaging: Miscellaneous Recent hospitalization: l Yes l No Delirium during hospitalization: l Yes l No Fall risk: l Yes l No Assistive device: l Yes l No
- 7. Performing a Cognitive Assessment and Developing a Care Plan in Primary Care1-4 Full abbreviations, accreditation, and disclosure information available at PeerView.com/XUM40 COGNITIVE IMPAIRMENT VISIT TEMPLATE Historical Data Allergies: Medical: Surgical: Family: (Dementia? Early or late onset?) Social: Tobacco/alcohol/drugs: l Yes l No ROS (circle pertinent findings) General: Patient denies fever or chills. Denies recent weight loss or gain. HENT: Denies headache or congestion. Denies hearing loss. Eyes: Denies blurry vision or double vision. Heart: Denies chest pain or palpitations. Lungs: Denies shortness of breath or cough. GI: Denies abdominal pain, nausea, vomiting, diarrhea, or constipation. GU: Denies dysuria, frequency, or hematuria. MSK: Denies weakness or edema. No falls. Neuro: Denies numbness or tingling. Heme: Denies abnormal bruising or bleeding. Physical Exam (circle pertinent findings) Vitals: Weight gain or weight loss: l Yes l No Comment: General: stated age, well developed, well-nourished, and in no apparent distress Skin: warm and dry w/o rash Eyes: PERRL, EOMI, conjunctiva clear Pharynx: posterior pharynx without erythema or exudate Neck: supple, no masses, no bruit Lungs: clear, no rales, rhonchi, or wheezes Heart: RRR without murmurs, gallops, or rubs Abdomen: soft, nontender, BS normal Musculoskeletal: no localized tenderness or swelling, full range of movement Page 4 Neurologic (circle pertinent findings): • CN • Motor • Sensory • Cerebellar • Reflexes • Gait • Tremor • Psych: alert, pleasant
- 8. Performing a Cognitive Assessment and Developing a Care Plan in Primary Care1-4 Full abbreviations, accreditation, and disclosure information available at PeerView.com/XUM40 Cognitive Assessment and Care Plan (CPT 99483) Template CACP_10: Written care plan Today’s date: Next follow-up date: Cognitive problems Actions ❑ None ❑ Mild cognitive impairment ❑ Mild dementia ❑ Moderate stage ❑ Late stage Type of dementia ❑ Alzheimer’s ❑ Vascular ❑ Mixed ❑ Lewy Body ❑ Frontotemporal ❑ Other ❑ Unknown; need further evaluation ❑ Advance care planning (living wills, family meeting) ❑ Additional diagnostic testing (check all that apply) ❑ Biomarker testing: ❑ Neuroimaging: MRI ❑ Neuroimaging: CT ❑ Neuroimaging: Amyloid PET ❑ Neuroimaging: Other ❑ Referral to neurologist/psychiatrist/ geriatrician: ❑ Aging in place planning vs assisted living ❑ Driving safely ❑ Exercise your body ❑ Exercise your brain (remediation, hobbies, games, computer, volunteering) Neurological, mental health, behavioral, functional problems ❑ Aggression ❑ Delusions ❑ Depression/suicide ❑ Hallucinations ❑ Decision making (capacity) ❑ Safety ❑ Sleep ❑ Alcohol avoidance ❑ Autonomy promotion ❑ Counseling ❑ Driving safety ❑ Environmental “rounds” ❑ Exercise ❑ Home safety ❑ Medications: antidepressants/antipsychotics/ anxiolytics/other: Medical problems ❑ Lung disease ❑ Heart disease ❑ Parkinson’s disease ❑ Vision and/or hearing ❑ Swallowing ❑ Cancer ❑ Dental ❑ Kidney disease ❑ Liver disease ❑ Gastrointestinal ❑ Urologic ❑ Other ❑ Cardiac rehabilitation ❑ Dental care ❑ Fall prevention ❑ Hearing/vision evaluation ❑ Hospice care ❑ Immunizations (flu, pneumococcal, tetanus booster, shingles) ❑ Incontinence ❑ Physical/occupational therapy evaluation ❑ Pulmonary rehabilitation ❑ Speech therapy evaluation ❑ Other: Caregiver assistance ❑ Adult day care ❑ Aging in place (home modification) ❑ Alzheimer’s Association ❑ Assistance from other resources (clubs, church, family, coworkers) ❑ Barriers to assistance ❑ Behavior management skills ❑ Communication skills ❑ Disease-specific resources ❑ Environmental management ❑ Home aides ❑ Hospice ❑ Healthy diet (dietician if needed, Meals on Wheels) ❑ Lab testing: CBC/CMP/TSH/B12/folate/RPR/ HIV/Other ❑ Legal/financial planning (power of attorney, guardianship, advance directives) ❑ Medication: donepezil/rivastigmine/galantamine/ memantine/donepezil + memantine ❑ Medication: aducanumab/lecanemab ❑ Medications to avoid (sleep aids, diphenhydramine) ❑ Social engagement (clubs, church, sports) ❑ Music therapy ❑ Reminiscence therapy ❑ Relaxation therapy (art, pets, yoga, muscle relaxation) ❑ Sleep patterns ❑ Structure ❑ Support group ❑ Other ❑ Legal/financial planning ❑ Memory/communication aids (clock, calendar, glasses, hearing aids, pictures) ❑ Medical/practical supplies ❑ Medication management ❑ Safety planning (guns, stairs, home hazards, falls) ❑ Self-care actions ❑ Senior alert system ❑ Support group 1. https://www.alz.org/media/Documents/Cognitive-Impairment-Care-Planning-Toolkit_012623.pdf. 2. Borson S et al. Alzheimers Dement. 2017;13:1168-1173. 3. Form adapted from https://www.aafp.org/fpm/2019/0100/p11.html. 4. https://Championsforhealth.Org/Wp-content/Uploads/2021/09/Alzheimers-project-booklet-v11-082221-web.pdf. Page 5
- 9. Disclosing a Diagnosis of MCI or Early Dementia1,2 Full abbreviations, accreditation, and disclosure information available at PeerView.com/XUM40 How NOT to Disclose a Diagnosis • Not planning enough time: A life-altering diagnosis cannot be rushed • Not involving family members – 73% of patients with dementia are unable to explain their diagnosis shortly after disclosure • Leading with the diagnosis: Must establish rapport and prepare the patient • Being definitive without evidence – These are complex neurologic puzzles – If there is uncertainty, seek more tests Pre-Disclosure • Plan >30 minutes for a diagnosis – There will be questions • Ask caregiver to accompany the patient – Caregivers play important role of supervision/support • Before you tell, ask; explore the patient’s perspective of the problems – Is there denial, wishful thinking, unrealistic expectations? – Does the patient have lack of insight (anosognosia)? • Reassure the family and the patient that you have heard all their concerns Disclosure Tips
- 10. Disclosing a Diagnosis of MCI or Early Dementia1,2 Full abbreviations, accreditation, and disclosure information available at PeerView.com/XUM40 • Setting the stage – Acknowledge the changes, demonstrate understanding – Use terms like memory “concerns,” “issues,” or “inefficiencies”; mirror their language – Consider avoiding trigger words like memory “problems” • Create confidence in the process and the thorough evaluation – Build the case; review the evaluations and purpose of each (eg, MRI, cognitive testing, specialist report) – Review objective cognitive data (“Not doing as well as you would have 5 years ago”) – No single test makes the diagnosis – It is okay to use terms like “working,” “possible,” or “probable” diagnosis – Suggest further workup is needed if picture is not clear • Disclose the diagnosis directly to the patient • Assess their understanding of the diagnosis • Respond empathetically Disclosure Tips After the Disclosure: Where Do We Go From Here? • Let’s go after it – Start meds (there are treatments) – Minimize contributing factors (eg, sleep, depressive symptoms) – Lifestyle: you can fight back (eg, exercise, eat right, stress reduction) • Foster hope – Focus on quality of life, well-being, and health promotion – Take trips sooner than later in earlier stages – Empowerment in research participation • Plan follow-up – A diagnosis is a process and does not end at that visit • Planning for the future – Discuss support services Cognitive care multidisciplinary team Be proactive rather than reactive 1. https://www.kumc.edu/documents/alzheimers/8-6-21-Tips-Dementia-Diagnosis.pdf. 2. https://www.psychiatrictimes.com/view/the-science-ethics-and-art-of-disclosing-a-dementia-diagnosis.