Downloaded 24 times
![About You
0 Experience with [any] CONCISE analysis 10](https://image.slidesharecdn.com/cpsi-incidentanalysislearningseries-module05-20130131-130225164058-phpapp02/85/Module-5-Concise-Analysis-Method-7-320.jpg)

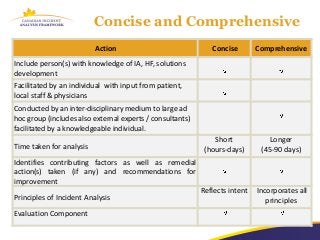
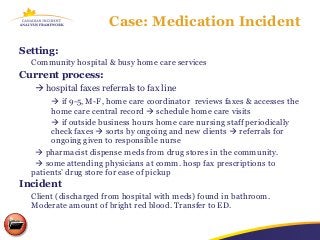
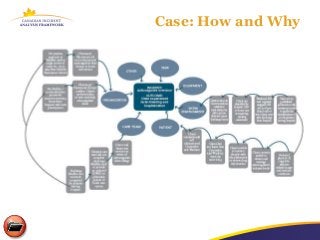
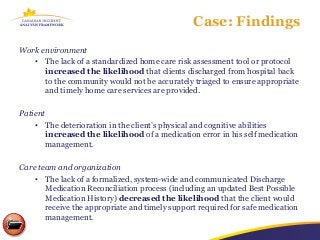
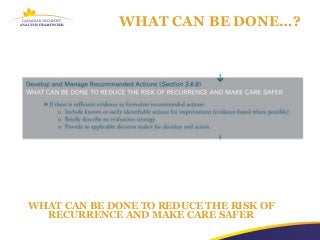
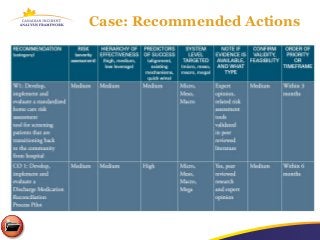
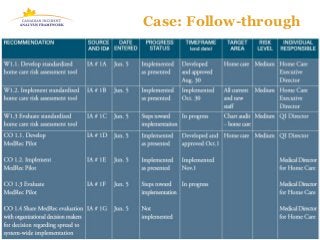


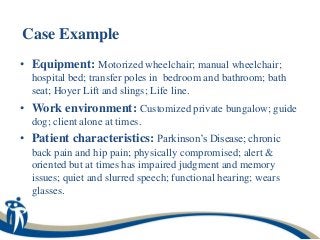





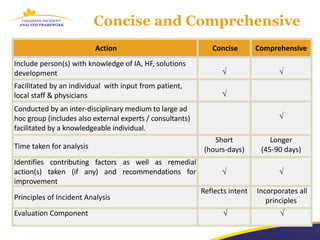
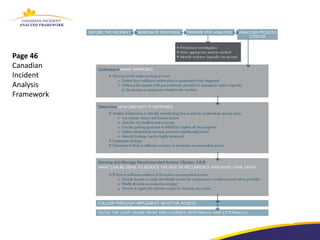
The document discusses a learning program on concise incident analysis, highlighting the method's significance, processes, and practical applications in healthcare settings. It outlines a case study of a medication incident that occurred in a home care context, analyzing factors contributing to the adverse event and proposing systematic recommendations for improvement. Emphasis is placed on interactive learning, knowledge sharing, and the incorporation of feedback to enhance patient safety and prevent recurrence of similar incidents.




![Product placements [In-Film Branding] and advertising in movies](https://cdn.slidesharecdn.com/ss_thumbnails/productplacementsinmovies-141208050624-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)



















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
















