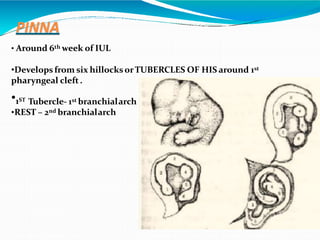
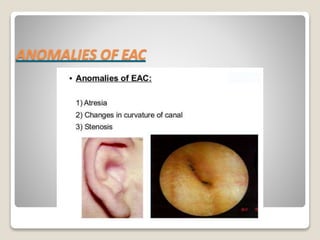
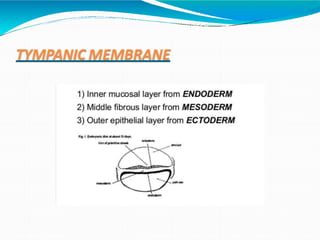
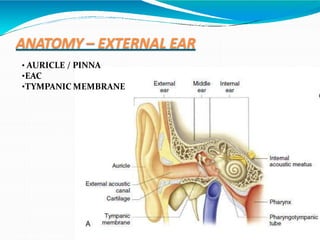
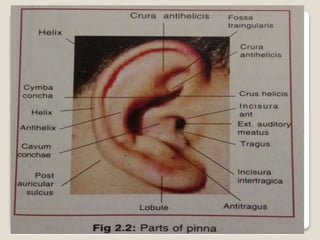
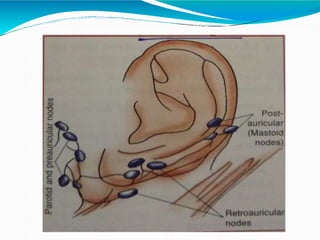
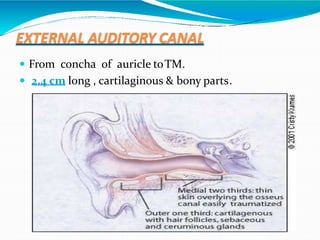
This document discusses the embryology, structure, blood supply, nerve supply, and clinical importance of the external ear. It begins with the embryological development of the pinna from hillocks and branchial arches. It describes the normal anatomy of the pinna, external auditory canal, and tympanic membrane. It discusses common anatomical variations and clinical relevance. The document provides a detailed overview of the external ear's development and key structures.