Downloaded 16 times
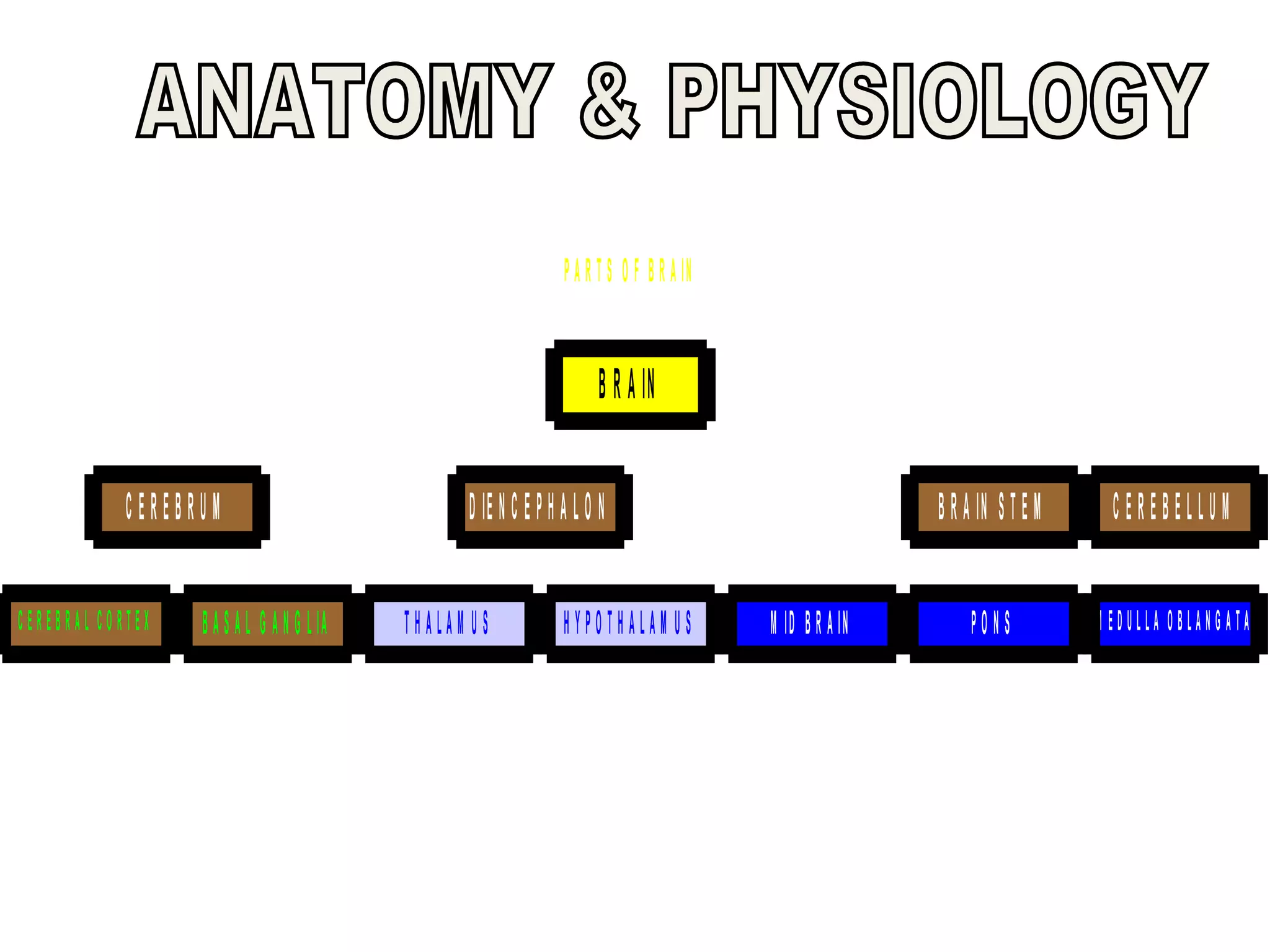
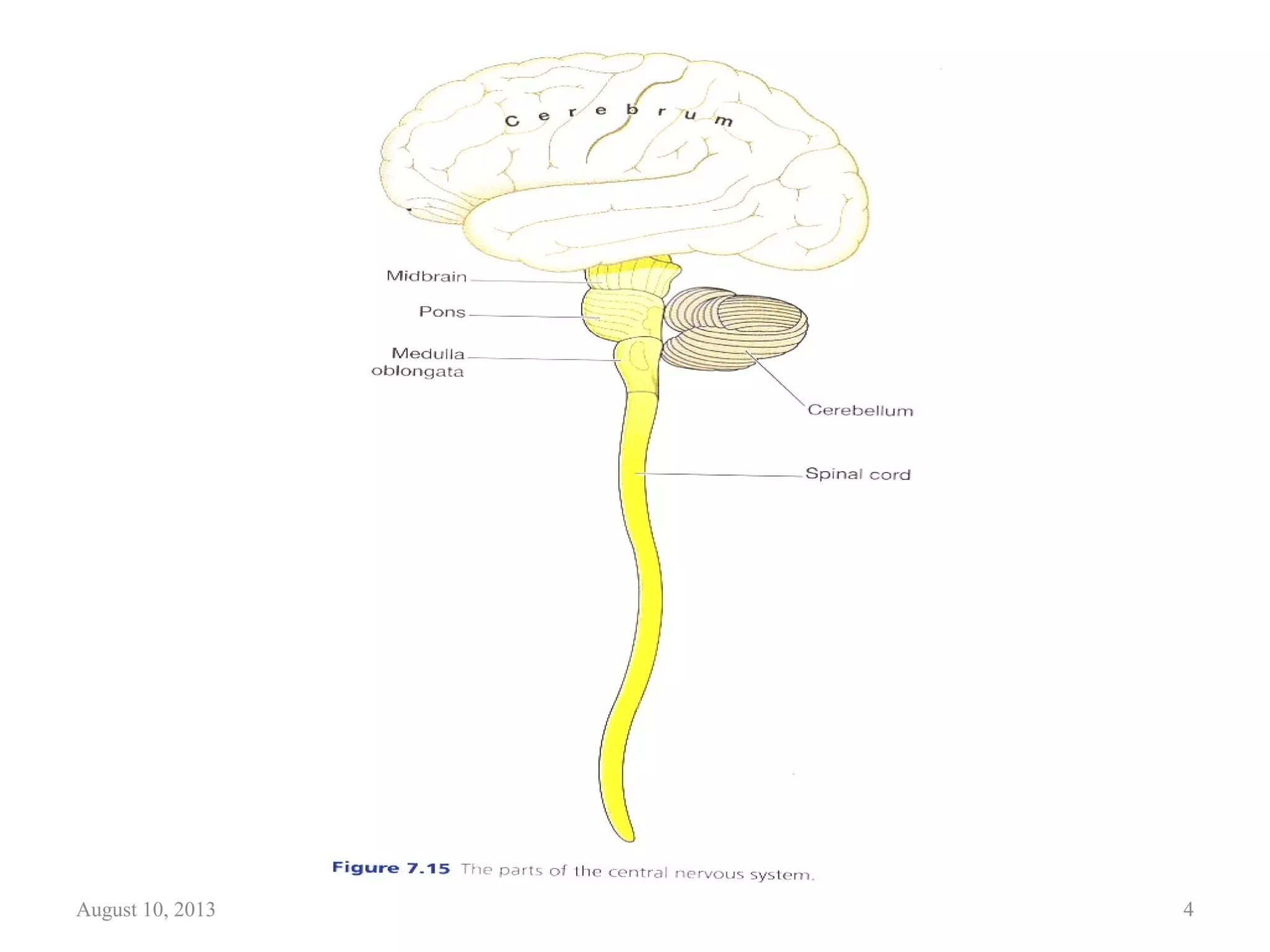
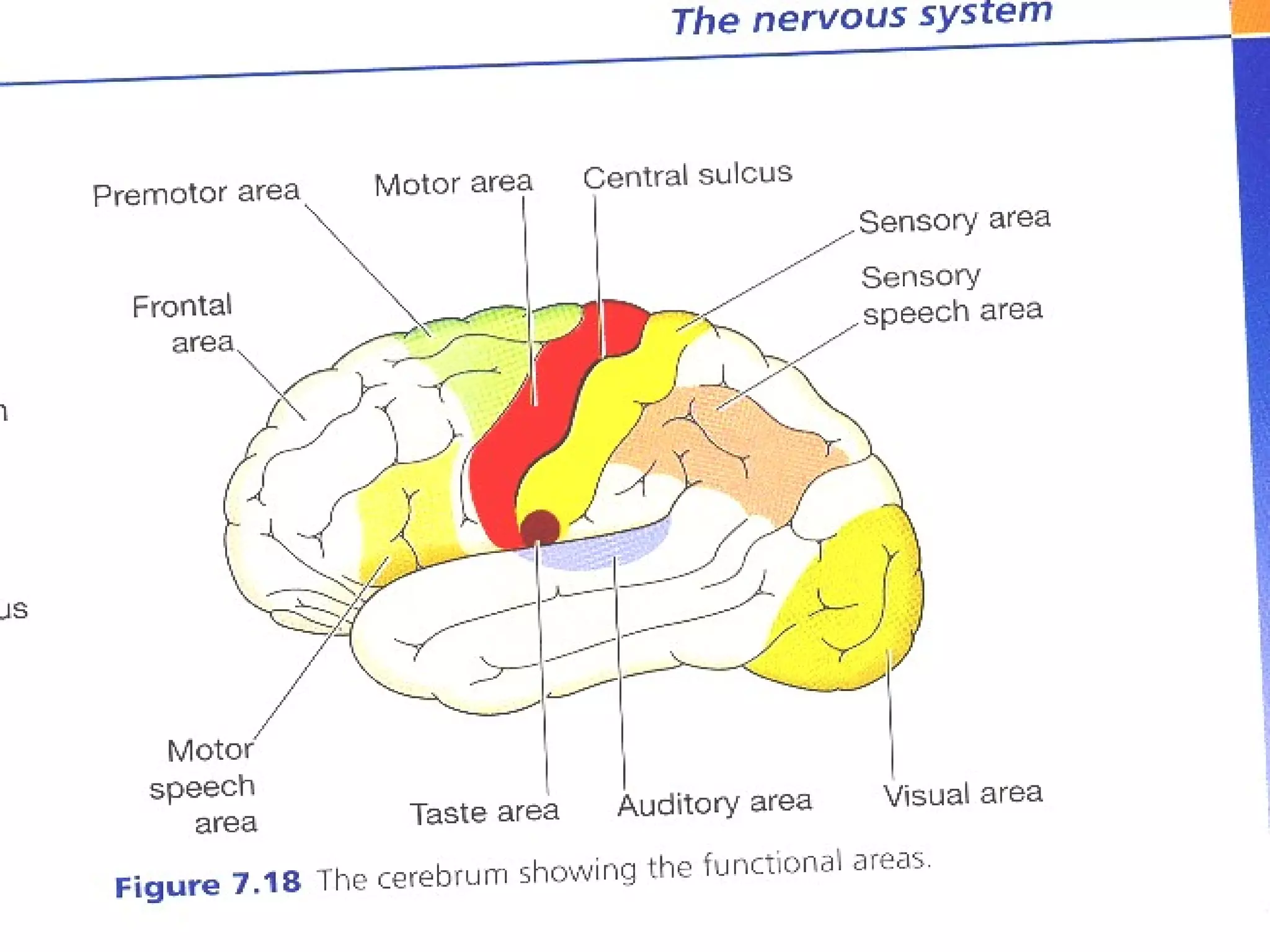










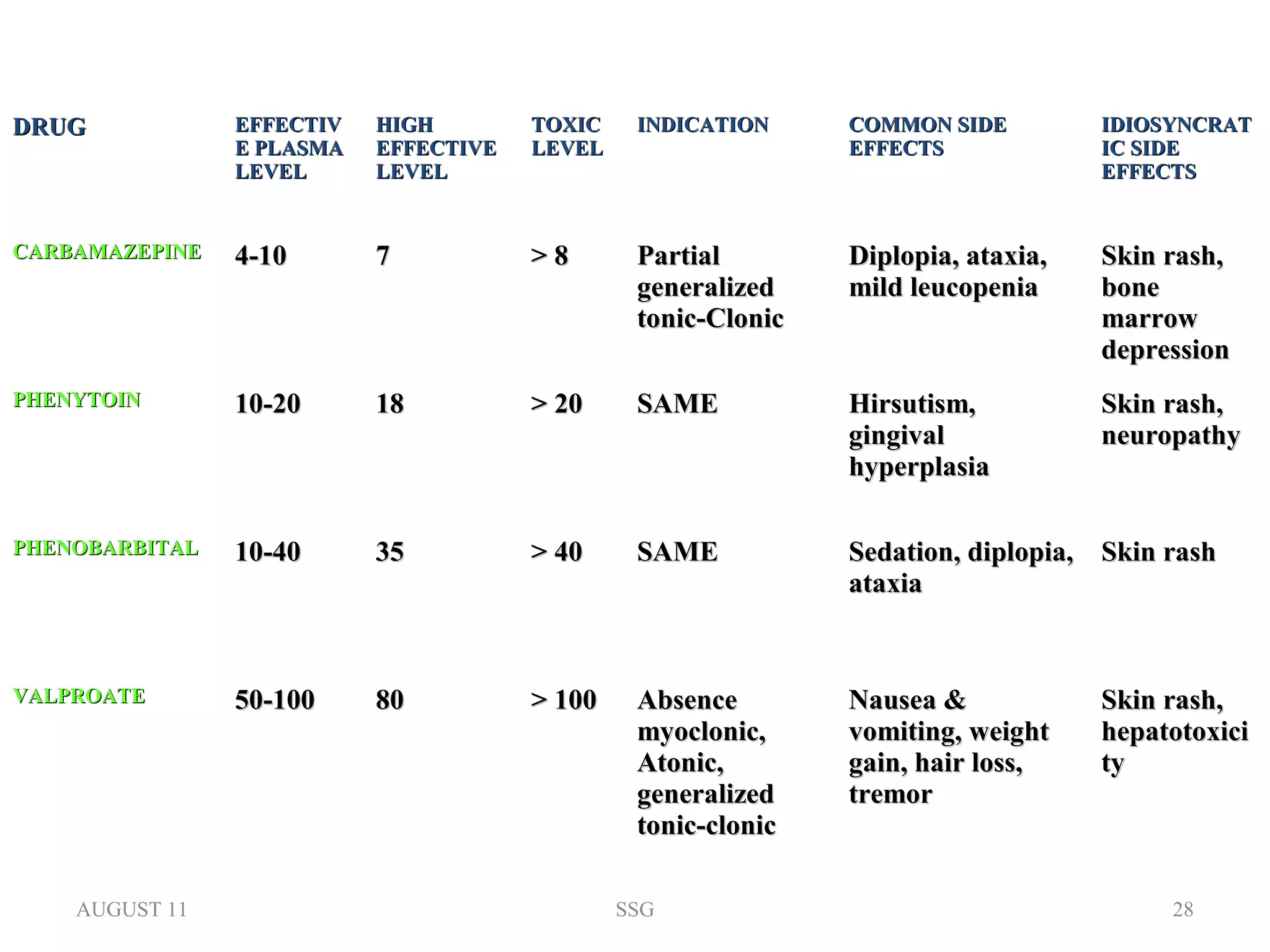








This document provides information about epilepsy including: - The parts of the brain involved in epilepsy like the cerebral cortex, basal ganglia, diencephalon, brain stem, and cerebellum. - The causes of epilepsy which can be structural, chemical, physiological, genetic factors, trauma, tumors, circulatory disorders, infections, and toxicity. - The types and phases of seizures including generalized, partial, simple partial, complex partial, tonic-clonic, absence, myoclonic and atonic seizures. - Common treatments for epilepsy including anti-epileptic medications like carbamazepine, phenytoin, phenobarbital and valproate.























![Epilepsy [Seizure disorders].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/epilepsynew-240129040418-51189c1c-thumbnail.jpg?width=640&height=640&fit=bounds)





































