DEFINITION
Episiotomy is surgicallyplanned incision given on
the perineum during second stage of labor to
enlarge the vaginal introitus, thereby facilitating
safe and easy delivery of the fetus.
3.
OBJECTIVES
To enlarge thesize of vaginal orifice
To prevent perineal tear
To reduce stress and strain on fetal head
To cut short second stage of labor
4.
INDICATIONS
Large fetus >4,000g
Preterm or small for gestational age baby in order to minimize
the risk of intracranial hemorrhage
Presence of rigid perineum
Face to pubis delivery, breech delivery or shoulder dystocia
In fetal distress, to make the delivery fast
When large lacerations seem inevitable
In case of operative delivery like forceps/ventose
Previous history of pelvic floor repair, perineal reconstructive
surgery
5.
TIMING OF EPISIOTOMY
Bulgingthinned perineum during contraction along
with bearing down efforts by the mother just prior
to crowning is the ideal time for giving episiotomy.
6.
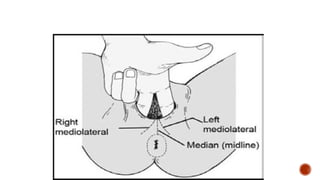
TYPES OF EPISIOTOMIES
Mediolateral: incision is given downward and
outward from the midpoint of fourchette.The cut
may be given either toward right or left side and
about 2.5 cm.
J shaped:The incisionstarts from the centre of
fourchette and directed posteriorly about 1.5
cm and then points downward and outward
along 5 or 7 o’ clock
11.
ADVANTAGES
MATERNAL BENEFITS
1. Clearincision is easy to repair
2. Healing is better than lacerated wound
3. Helps cut short the second stage of labor
4. Lessens the chance of trauma to the pelvis floor muscles
5. Tear may be avoided
6. There is less stretching of and less damage to the
bladder, anterior vaginal wall and urethra
REPAIR OF EPISIOTOMY
Requirement
Provide lithotomy position
A good source of light is needed
Instruct the mother to spread the thighs
Clean the perineal area with antiseptic solution
Drape the patient properly under aseptic precaution
Evacuate the uterine cavity for retained clots or placenta
Vaginal pack may be inserted and placed high up, if the wound site is
obscured by oozing of blood from above, but it must be documented and
removed , else it may lead to sepsis
16.
Suture material
Dexon ornumber ‘0’ chromic catgut is usually used to repair
episiotomy. It is an absorbable suture and is spontaneously
sheds off after 7-8 days of repair. Silk or nylon
(nonabsorbable) sutures may be used and removed on 6th
day.
17.
EPISIOTOMY SUTURING
Thesequence of episiotomy suturing is as follows:
a) Vaginal mucosa: it is sutured first. First inspect the apex of
tear and first suture is applied just above the apex.
Continuous suture is used to repair vaginal mucosa from
above downward till the fourchette is reached.
b) Perineal muscles: Interrupted sutures are used to repair
perineal muscle same from above downward till the
fourchette is reached.
c) Skin : Mattress suture or figure of eight is used to repair skin.
18.
EPISIOTOMY CARE
Maintenanceof perineal hygiene: instruct to clean episiotomy
wound after every urination and defecation.
Provide perineal care twice daily and clean the episiotomy
wound with antiseptic solution
Assess the wound healing status every time with REEDA scale
If there is impaired wound healing, provide sitz bath using
MgSO4, moist and dry heat therapy or use analgesic drugs/
antibiotic therapy
Do not sit with cross legs because stitches may break
19.
Instruct the motherto ambulate to avoid stretch on the
perineal wound
If nonabsorbable sutures are used, stitches are removed
on 6th
day.
Advise the mother for abstinence for 6 weeks after
delivery.