













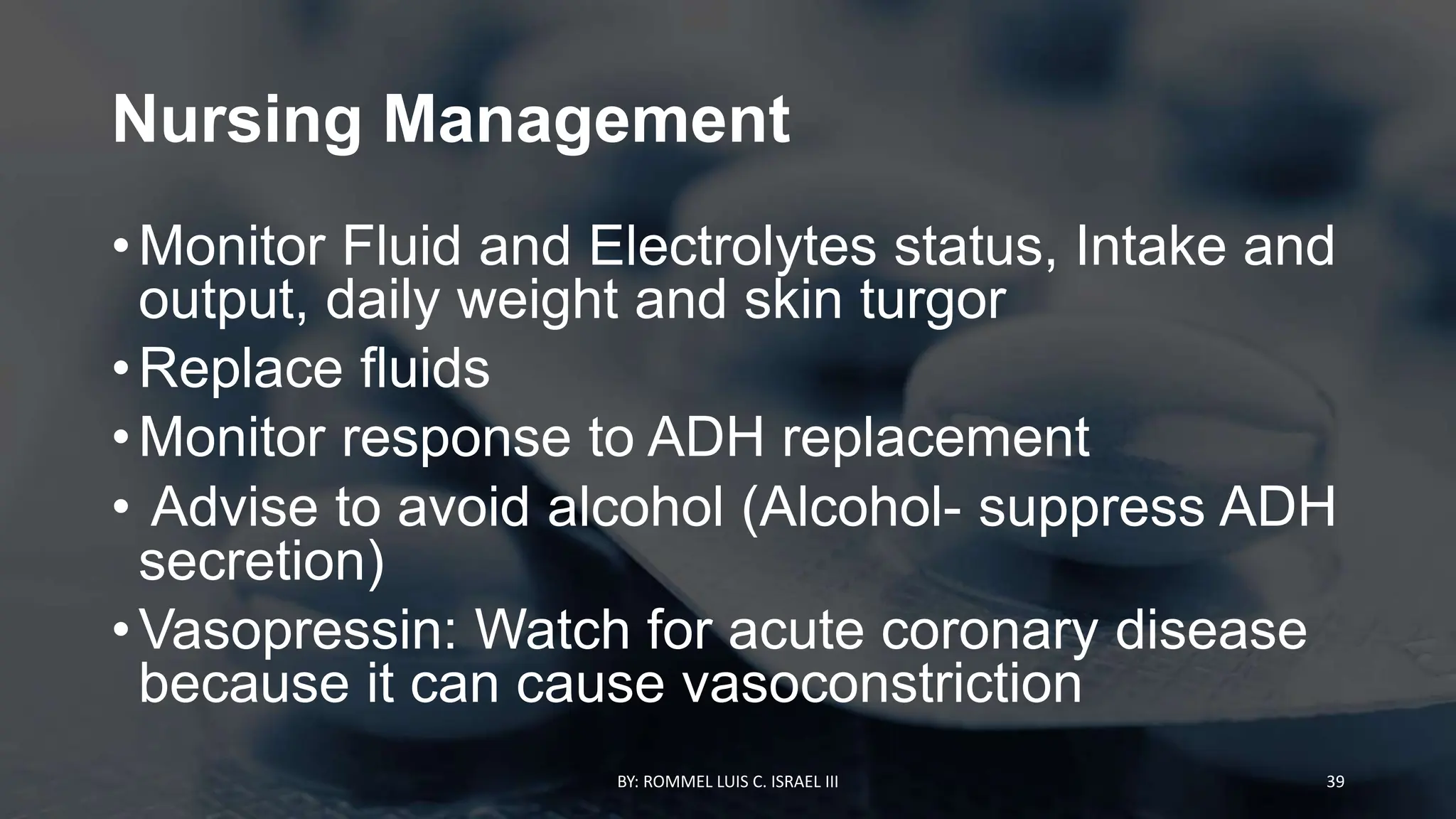
![Possible causes
BY: ROMMEL LUIS C. ISRAEL III 32
Cerebral
vascular
accident (CVA)
Hypothalamic-
pituitary
tumors
Cranial trauma
or surgeries
Hereditary
Drugs (lithium
and phenytoin
[Dilantin])
Alcohol
(transient DI)](https://image.slidesharecdn.com/endocrineassessment-231007104430-3ac68699/75/ENDOCRINE-ASSESSMENT-pptx-32-2048.jpg)









































![Nursing
Interventio
ns
BY: ROMMEL LUIS C. ISRAEL III 83
Provide adequate rest.
Administer sedatives as
prescribed.
Provide a cool and quiet
environment.
Obtain weight daily.
Provide a high-calorie
diet.
Avoid the administration
of stimulants.
Administer antithyroid
medications(propylthiour
acil [PTU]) that block
thyroid synthesis, as
prescribed](https://image.slidesharecdn.com/endocrineassessment-231007104430-3ac68699/75/ENDOCRINE-ASSESSMENT-pptx-83-2048.jpg)


















































































This document provides a comprehensive overview of endocrine assessment, including both normal and abnormal findings, with emphasis on the necessary history-taking, physical examination techniques, and symptomatology associated with endocrine disorders. It also discusses specific conditions such as diabetes insipidus and various forms of pituitary dysfunction, detailing clinical assessments, therapeutic interventions, and nursing management strategies. The document highlights the importance of medication management, patient education, and monitoring for complications during endocrine disease treatment.