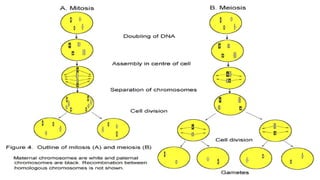
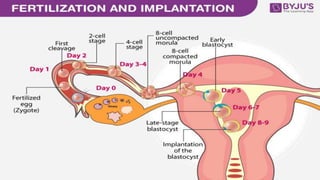
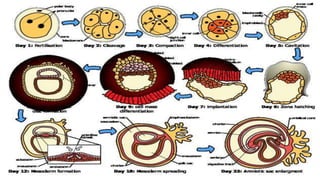
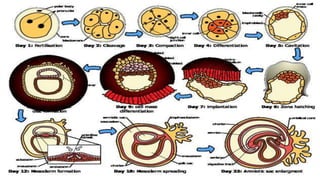
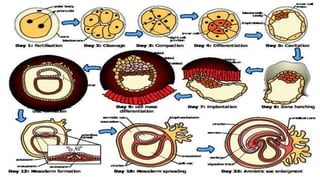
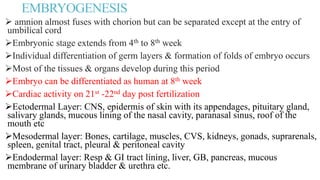
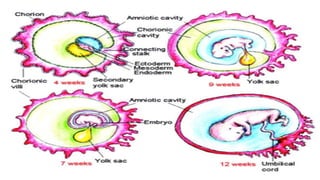
This document summarizes key stages in human fertilization and embryogenesis. It describes gametogenesis including oogenesis and spermatogenesis, the maturation of egg and sperm cells. It then explains ovulation, fertilization, formation of the morula and blastocyst. Implantation of the blastocyst in the uterine wall and subsequent embryogenesis, including the formation of germ layers and development of organ systems, is also outlined.