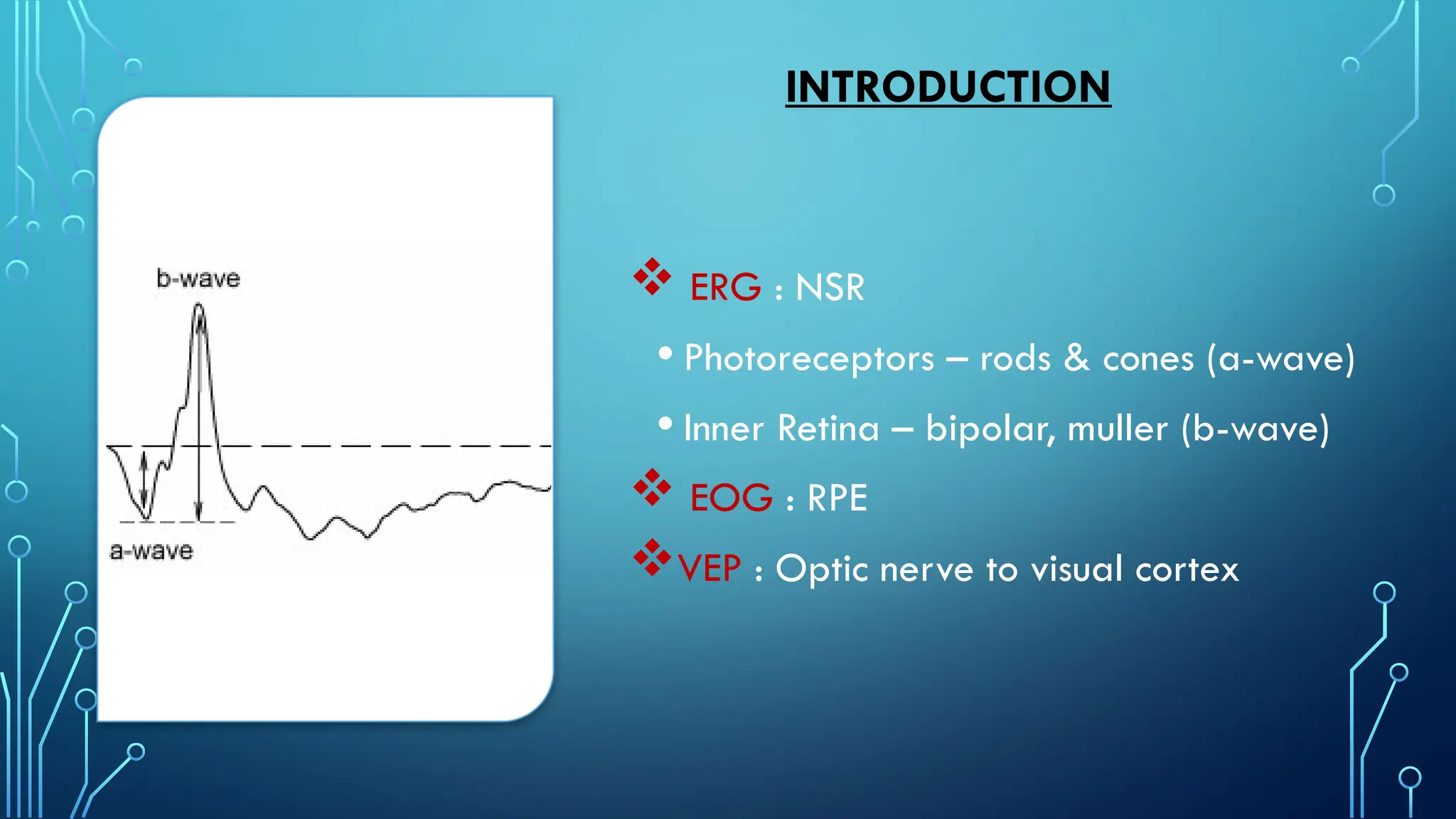
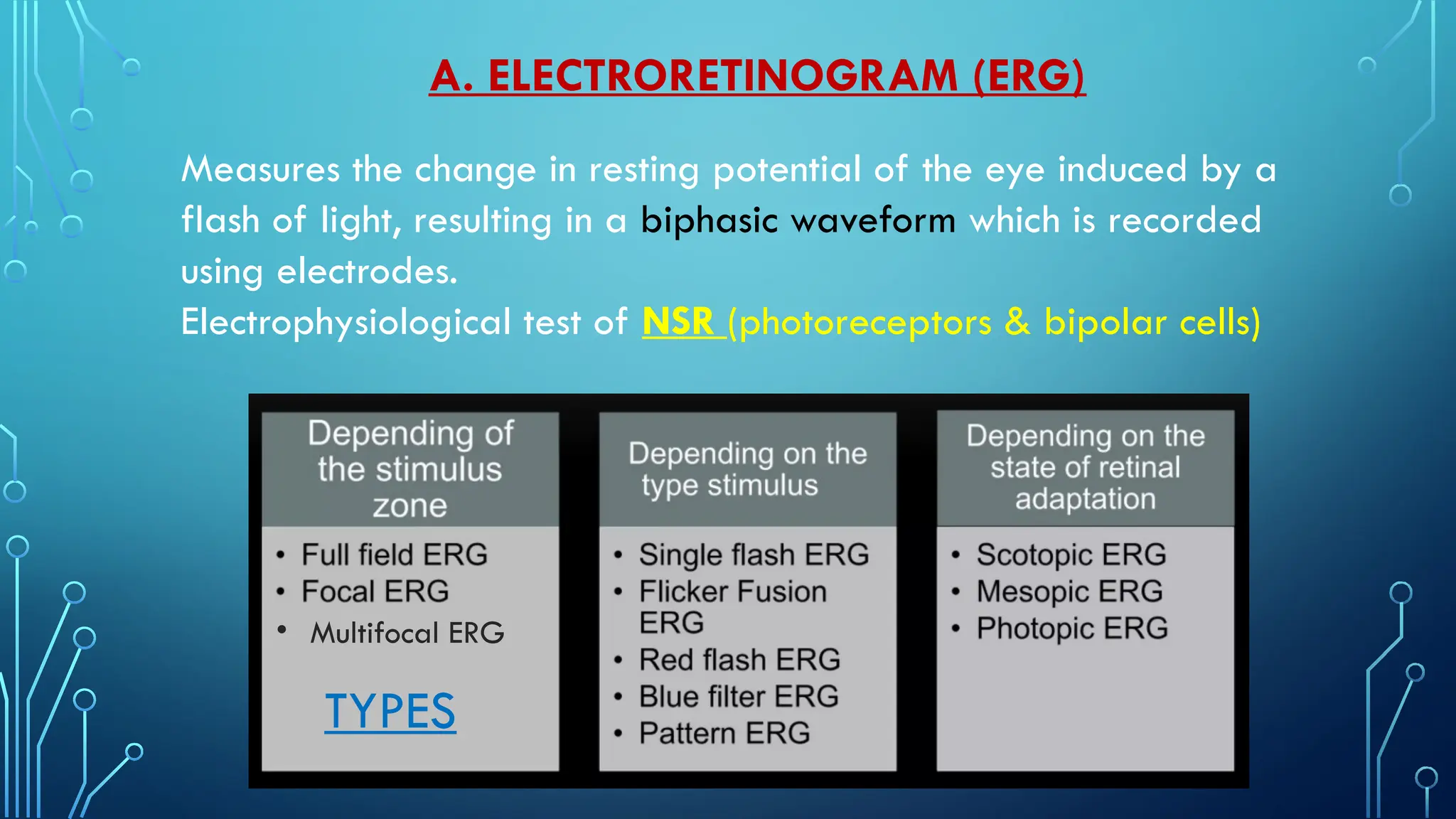
The document discusses various electrophysiological tests used in ophthalmology, including electroretinogram (ERG), electro-oculogram (EOG), and visual evoked potential (VEP), describing their types, waveforms, and clinical indications. It highlights the significance of these tests in diagnosing retinal and optic nerve conditions, along with the physiological factors that can affect their results. Additionally, the document details the methodology for performing these tests, typical abnormalities observed, and their relevance in differentiating between ischemic and non-ischemic retinal diseases.