Downloaded 28 times











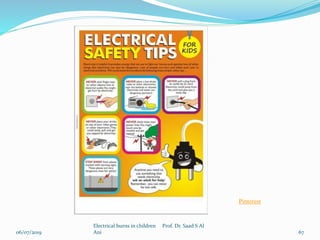



The document discusses electrical burns in children, categorizing them into three types: minor burns, high-tension wire burns, and lightning burns, detailing their causes, effects, and management options. It underscores the dangers associated with electrical exposure, including potential cardiac and neurological complications, and emphasizes the importance of safety precautions in preventing such injuries. Additionally, the document includes an electrical safety quiz to educate about safe practices around electricity.




































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)








![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)









