2
Introduction
• The bloodsupply to the inner layers of the retina is derived entirely
from the central retinal artery unless a cilioretinal artery is present.
• Retinal ischemia results from disease processes that affect the vessels
anywhere from the common carotid artery to the intraretinal arterioles.
• The signs and symptoms of arterial obstruction depend on the vessel
involved: occlusion of a peripheral arteriole may be asymptomatic,
whereas an ophthalmic artery occlusion can cause total blindness.
Central retinal artery
•First branch of Ophthalmic Artery
• Arises near optic foramen and
courses ahead as
outside optic nerve
in sub arachnoid space
centre of optic nerve
optic nerve head
in Retina
5.
Outside optic nerve; runs a wavy course forward , below optic nerve , adherent to dural
Sheath about 10-15 mm behind eyeball , bends upwards to pierce dura and
Arachnoid
Subarachnoid space ; again bends upwards at right angle and invaginates
Pia to reach centre of optic nerve
Centre of optic nerve ; passes anteriorly and pierces lamina cribrosa to
Appear inside the eye
Optic nerve head ; lies superficially in nasal part of physiological cup , divides into
Superior and nasal branch and subdivides into temporal and nasal branch
6.
In retina :the four terminal branches they
divide dichotomously as they proceed
towards ora serrata
10
Epidemiology
• 1-2 casesin 100,000 people per year
• Older adults (early 70s)
• Men> Women
• 1-2% B/L
• Comorbidities: HTN,DM, Smoking, Lipid disorder
• The life expectancy of patients with central retinal artery occlusion
(CRAO) is significantly lower (5.5 years) compared to an age-
matched population without CRAO (15.4 years).
Reference - Retinal artery occlusion epidemology
14
Mechanisms of Occlusion
Embolic
80%
•Either from carotid or heart
• More common cause
• Site of obstruction is usually at the
site where the CRA pierces the dura
matter around the optic nerve
Thrombotic
20%
• Due to atherosclerosis
• Less common than embolus
• Site of obstruction is mainly at the
lamina cribrosa
23
Cherry-red spot appearanceof foveola , as foveola is nourished by the choroidal
circulation
NFL & inner retina opacified, more denser in the posterior
pole as a result of increased NFL thickness
25
Clinical features
• Symptoms:
Sudden,severe, painless (except in GCA), unilateral visual loss,
occurring over seconds
History of amaurosis fugax (10%)
Relapsing and remitting course of visual loss (in arterial spasm)
26.
26
• Signs:
VA: CFto light perception (>90%)
VA of NPL usually suggests either GCA or ophthalmic artery
obstruction
Afferent pupillary defect
Anterior segment: Normal unless rubeosis develops
27.
27
Factors responsible forvisual prognosis
Duration of retinal ischemia
• Complete recovery can occur if ischemia reversal & reperfusion
started in 90 minutes
• Some improvement possible upto 240 min (4 hours)
• Beyond that irreversible , massive damage occurs
28.
28
Types of CRAO
•Transient NA-CRAO :Best improvement, can improve by 82%
• NA-CRAO with cilioretinal artery sparing : can improve by 67%
• NA-CRAO : can improve by 22 %
• Arteritic CRAO : no improvement possible
source : Central retinal artery occlusion, Hayreh, Sohan Singh (10.4103/ijo.IJO_1446_18)
29.
Fundus examination
• Maybe normal during the 1st
hour
Subsequently, posterior pole becomes opaque and edematous
except the foveola
Cherry red spot macula: Pale retina with reddish hue of fovea.
Box-carring or segmentation of the blood column in the
arterioles(cattle trucking)
• Occasionally, cilioretinal artery sparing is evident – part of macula
remains normal in colour.
30.
30
Chronic stages ofCRAO (As retina
recovers)
Retina opacification
disappears
Arterial
attenuation in
58%
Optic atrophy in
91%
Cilioretinal
collaterals in 18%
Pigmentary
changes at macula
11%
1 month
3 month
32
FFA
ACUTE CRAO
• InNA CRAO- sluggish filling of
the retinal vasculature , & a
variable amount of residual
circulation
• Transient CRAO – almost
normal retinal circulation
• In arteritic CRAO- evidence of
posterior ciliary artery occlusion
LATE CRAO
• Complete restoration of retinal
arterial circulation(except for the
delayed arm to retina time)
within a few days to several
weeks of a CRAO
36
• Visual field
–Central scotoma –most common
– Paracentral scotoma
– Improve in 28% , remain stable in 57% and worsen in 7%
• Electroretinogram
– Inner retinal layers are more affected :↓ B-wave more than A-wave
– Ophthalmic artery occlusion: attenuation of both A wave & B wave due to
global ischemia
37.
37
Systemic work up
•History-medical,drugs,ocular disease
• Blood pressure
• Blood tests:
• FBS, HbA1c,CBC with differentials,platelets,
• PT/PTT,ESR
Lipid profile,serum homocysteine level,
ANA,FTA-ABS,VDRL or RPR
• Hb electrophoresis,cryoglobulins
• Coagulation profiles
38.
38
• HS-CRP,lipoprotein(a)
• AntiphospholipidAbs,lupus anticoagulant
• Sr,protein electrophoresis
Complete medical evaluation with careful attention to CVS disease or
hypercoagulability
ECHO,transesophageal echocardiography (TEE)
Carotid & vertebral doppler
Magnetic resonance imaging (MRI) including diffusion weighted imaging
(DWI) is the preferred imaging modality
42
• Hyperosmotic agents.Mannitol or glycerol have been used for their
possibly more rapid IOP-lowering effect as well as increased
intravascular volume.
• Sublingual isosorbide dinitrate
• Transluminal Nd:YAG laser embolysis/embolectomy
• Thrombolysis
43.
43
Systemic Management FollowingRetinal
Artery Occlusion
• Urgent referral to a specialist stroke clinic is advisable
• General risk factors as discussed above should be addressed and
smoking should be discontinued.
• Antiplatelet therapy
• Oral anticoagulation (e.g. warfarin) : Atrial fibrillation
• Carotid endarterectomy : indicated in patients with symptomatic
stenosis greater than 70%.
• Obstruction associated with temporal arteritis: High-dose
corticosteroids
44.
44
On Follow Up
•Follow as directed by managing internist and/or neurologist.
• Repeat eye examination in 1 to 4 weeks, checking for
neovascularization of the iris/disc/angle/retina (NVI/NVD/NVA/NVE)
• Photocoagulation: Iris neo-vascularization
• Long-term management aims are to identify and address the
underlying cause in order to prevent further ischaemic events (e.g.
investigate and treat hypertension and reduce risk factors for
atherosclerosis) and low-dose aspirin may be beneficial.
45.
45
Prevention
• Raising awareness“BE FAST”
• Warning sign : amaurosis fugax.
• Some basic first aid measures should be explained to the patient :
ocular massage , breathing in a bag
• Patient can be instructed to sublingial sorbitrate or use a nitroglycerin
patch
• Report to an ophthalmologist without any delay
46.
46
Prognosis
• Vision remainsstable ( unless associated with NVG)
• Risk of cerebral stroke is high
• Life expectancy after CRAO : 5.5 years compared to 15.4 years for an
age-matched population
• For patient with visible emboli , the mortality rate is 56% for the next
9 years compared to 27% for an age matched population
47.
47
Intravenous Thrombolysis WithLow-dose
Recombinant Tissue Plasminogen Activator
in Central Retinal Artery Occlusion
“American Journal of Ophthalmology, August-2008”
• Purpose:
To evaluate the beneficial effect of intravenous thrombolysis aiming at
rapid restoration of blood flow during the early hours of a central retinal
artery occlusion (CRAO).
• Conclusions:
Thrombolytic treatment with intravenous low-dose rt-PA is of value for
an improved visual recovery in patients with acute CRAO, if
administered within the first 6.5 hours after the onset of symptoms.
48.
48
European assessment groupfor lysis in the
eye (EAGLE)
• In 2010 the EAGLE study group published the results of the first
prospective, randomized clinical trial evaluating the effect of local intra-
arterial fibrinolysis (LIF) using recombinant tissue plasminogen activator
(rtPA) compared with conservative treatment(CST) for acute non arteritic
CRAO.
• At 1 month, the mean best-corrected visual acuity improved significantly
in both groups (60% among CST and 57.1% among LIF)
• Adverse reaction was noted in 4.3 % in CST group and 37.1% in LIF
group.
• In light of these 2 therapies,similar outcomes and the higher rate of adverse
reactions associated with LIF, we cannot recommend LIF for the
management of acute CRAO.
50
Branched retinal arteryocclusion
• An abrupt diminution of blood flow through one or more
of the branches of central retinal artery causing ischemia
of the inner retina of the supplied territory
Epidemiology
• Less common than CRAO
• Mean age: 60 years
• M>F=2:1 above 50 years, but equal in below 50 years
• Laterality: R>L=60:40
• More incidence in temporal retina than nasal
51.
51
Etiopathogenesis
• More than2/3rd
of cases are due to emboli
• Risk factors:
Non-modifiable: Positive family history , race, ethinicity
Modifiable:
Hypertension
Elevated lipid levels
Cigarette smoking
Diabetes mellitus
52.
52
Clinical features
• Symptoms:
Abrupt, painless loss of vision in the visual field corresponding to the
territory of the obstructed artery(altitudinal or sectoral field loss)
Amaurosis fugax in about 1/4th
of patients
• Signs :
VA is variable
Intact central visual acuity in about 50% of patients
RAPD may be present, but determined by extent of retinal
involvement
53.
53
Fundus examination
• Retinalwhitening, resulting from oedema corresponding to the area
of ischemia
• Retinal emboli can be seen
• Flame shaped hemorrhages at the margin of ischemia may be
present
• Narrowing of arteries and veins with segmentation of blood
column.
54.
54
Contd…
• In chroniccase, loss of the nerve fiber layer in the affected area may
be apparent
• Arteriolar collaterals on the optic disc or at the site of obstruction may
develop
55.
55
Diagnosis
• Mainly clinical,based on history and clinical findings
• FFA
Will show non perfusion distal to the site of embolus or obstruction
Extreme delay of arterial phase
Late staining or even leakage from the embolus site and arterial walls
56.
56
Investigation
• FFA: usefulin diagnosis
• Goldman Perimetry: will show
the extent of visual field loss
• Other investigations for risk
factors as in CRAO should be
done
58
Treatment
• No provedtreatment
• Ocular massage or paracentesis may be successful in dislodging an embolus
• Laser photocoagulation has been employed to 'melt' an embolus, without
improvement in the vision
• systemic anticoagulation may prevent further events in patients with
coagulopathy
59.
59
Course and outcome
•Most patients remain with a fixed visual field defect, but intact central
acuity
• About 80% of eyes recover to 6/12 or better central acuity
• Retinal neovascularization has been reported, but uncommon
• Iris neovascularization does not occur
60.
60
Branch Retinal ArteryOcclusion: Visual
Prognosis
July 2008,American Journal of Ophthalmology
• Purpose : To evaluate the visual prognosis in eyes with branch retinal
artery occlusion (BRAO).
• Conclusions: Visual prognosis after BRAO seems to be correlated to
presenting VA. Eyes with initial VA of 20/40 or better usually
remained at 20/40 or better. Individuals with poor VA of 20/100 or
worse generally did not show the significant improvement reported in
previous studies.
61.
61
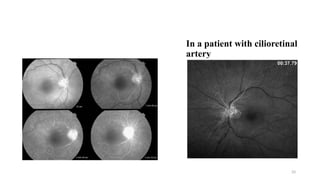
Cilioretinal artery obstruction
•Presents in 18-32% of population and arises from
posterior ciliary circulation.
• Supplies the macula and papillomacular bundle.
• Cilioretinal arteries enter on the temporal aspect
of optic disc
• Cilioretinal artery obstruction appears as areas of
superficial retinal whitening along the distribution
of these vessels
62.
62
Clinical variants
• Isolatedcilioretinal obstruction (40%)
In young individuals with
A systemic vasculitis
Usually good prognosis
63.
63
Cilioretinal obstruction withCRVO (40%)
Generally behaves as a nonischemic central
retinal vein obstruction with a good central
visual prognosis.
The scotoma from the artery obstruction is
usually permanent.
Cilioretinal artery obstruction with ischemic
optic neuropathy (15%)
Affects patients with giant cell arteritis
Carries good prognosis
64.
64
Ophthalmic artery obstruction
•Very rare,5% of patients with apparent CRAO
have in reality an acute ophthalmic artery
occlusion.
• Causes:
Associated local orbital or systemic diseases,
which include orbital mucormycosis, orbital
trauma, retrobulbar anesthesia, depot
corticosteroid injection, atrial myxoma, or carotid
artery disease.
Funduscopy; Intense retinal opacification
resulting from inner and outer retinal ischemia.
65.
65
• OAO canbe differentiated clinically from CRAO by the following
features:
Severe visual loss - bare or no light perception.
Intense ischemic retinal whitening that extends beyond the macular
area.
Little to no cherry-red spot.
Marked choroidal perfusion defects on fluorescein angiography.
Non-recordable electroretinogram.
Late retinal pigment epithelium alterations.
66.
66
Combined Artery AndVein Obstructions
• Central retinal artery obstruction combined with
simultaneous central retinal vein obstruction
rarely occurs.
• Present with acute, severe loss of vision, usually
to no light perception.
• The visual prognosis is generally poor
• the risk of neovascularization of the iris is about
75%
67.
67
Cotton wool spots
•Acute obstruction in the distribution of the radial
peripapillary capillary net leads to the formation of an
NFL infarct, or CWS, which causes impaired
axoplasmic transport in the NFL
• These inner retinal ischemic spots are superficial, white,
and typically 1/4th
disc area or less in size
• They usually fade in 5–7 weeks, although spots present
in association with DR (MCC) often remain longer
68.
68
• Fluorescein angiographydemonstrates a lack of filling of the capillaries
in the area of the cotton-wool spot, although this appearance may be due
in part to masking by the overlying opaque retina
• OCT
69.
69
Paracentral acute middle
maculopathy(PAMM)
•In patients with partial or incomplete CRAO,
ophthalmoscopy may show a more subtle and non-diffuse
retinal whitening in the middle layers of the perifoveal
macula, with peri-arterial sparing.
• This pattern of ischemia, known as paracentral acute
middle maculopathy (PAMM),
• The primary etiology in PAMM may be ischemia of the
deep capillary system
• The typical presentation is acute onset of diminished
central visual acuity or paracentral scotoma.
71
Arterial macroaneurysm
• Retinalarterial macroaneurysms are acquired ectasias of the first 3
orders of retinal arterioles.
• Large macroaneurysms can actually traverse the full thickness of the
retina.
• Vision loss may occur from embolic or thrombotic occlusion of the
end arteriole (white infarct) or from hemorrhage in any retinal layer.
• Often, there are multiple arterial macroaneurysms, although only 10%
of cases are bilateral.
72.
72
• Arterial macroaneurysmsare associated with systemic arterial
hypertension in approx. 2/3rd
of cases
• Typically, the macroaneurysm closes and scleroses spontaneously,
with accompanying resorption of related hemorrhage
• Initial management is usually observation. In most instances, closure
can be achieved with moderate- intensity laser treatment of the retina,
performed immediately adjacent to the macroaneurysm
#3 Centra retinal artery enters optic nerve 8-15mm behind the globe to supply retina
Preaxial system (6 branches of ICA)
Ophthalmic artery
Long PCA
Short PCA
Lacrimal artery
CRA
#6 Nasal branches run relatively straight course towards ora serrata compared to temporal branch which arch over the fov
#7 Parts of optic nerve=intraocular part (superficial nerve fiber layer,prelaminar,lamina cribrosa,retrolaminar ),intraorbital part,intracanalicular,intracranial layer
Surface nerve fiber layer(innermost layer) – central retinal artery branches-arterioles,sometimes supplied by cilioretinal artery
Prelaminar - short posterior ciliary artery
Laminar –SPCA and anastomosis called artery circle of zin haller
Retrolaminar – both central retinal SPCA ,plial plexus
CRA- centrifugal branches(towards)
And SPCA giving centripetal branches
#8 Terminal fundus arteriole bends to form superficial and deep capillary network.
Superficial capillary network lies BETWEEN NERVE FIBER AND the GCL
Intermediate capillary plexus lies at the inner edge of inner nuclear layer.
Deep lies BETWEEN INL & OPL
#9 15 to 20 % of people (18-32 % :AAO)
-Originate in a hook shape manner in temporal part of the disc, runs towards the macula and supplies it.
CAN SUPPLY A TINY AREA OF PERIPAPILLARY RETINA/ ½ OF ENTIRE RETINA
FFA is diagnostic-fills the concurrently with the filling of the choroid & choroid & usually before the start of filling of the CRA
-in case of complete artery occlusion it prevents patient from complete blindness
#14 There are 5 mechanism of occlusion of retinal arteries
#16 A. calcific embolus at the disc
Calcific 10%-15.5%=large,dull grey yellow white-a/w more severe obstruction, arising from diseased cardiac valves
B.fibrin-platelet emboli associated with arteriosclerosis
Thrombus 15%=platelet fibrin plaques-large white,mobile multiple, large-vessel arteriosclerosis
#17 C.Hollenhorst plaque located at arterial bifurcation
Cholesterl/Hollenhorst plaques =refractile,yellow orange crystals at bifurcation site, arising in the carotid arteries
D.Fat/bacterial vegetations/tumor/amniotic fluid
#21 Hayreh & Zimmerman discovered published article in 2024
A central retinal artery obstruction occurs when the blockage Is within the optic nerve substance itself and therefore the site of obstruction is generally not visible on ophthalmoscopy. Blockage at the level of the lamina cribrosa
SUPPLIES INNER 6 LAYERS
END ARTERY AS IT DOES NOT HAVE ANY ANASTOMOSIS
AION is located anteriorly to the lamina cribosa and is most likely caused by posterior ciliary artery occlusion while Posterior ION (PION) is posterior and results from improper pial vessel supply. Central retinal artery occlusion (CRAO) is a result of emboli and globe compression resulting in a loss of blood supply of the surface layer of the optic disk. Corneal abrasion (CA) is due to inhibition of corneal reflex and decreased tear production.
#22 Obstruction of the central retinal artery results in inner layer edema and pyknosis of the ganglion cell nuclei.
#23 Because of the contrast from the surrounding opacification & also due to RPE & choroid which lines through it
The opacity is most dense in the posterior pole as a result of the increased thickness of the nerve fiber layer and ganglion cells in this region.
The late stage shows a homogenous scar replacing the inner layer of the retina.
#25 Greek work amaurosis= dark and fugax= fleeting
Transient loss of vision in one or both eye due to lack of blood flow to retina
Dd of amaurosis fugax=TIA,stroke,CRAO,BRAO,CRVO,atherosclerosis of ICA,migraine,optic neuritis,papilledema,intracranial mass,hemorrhage,glaucoma,partial epilepsies,sickle cell disease
#26 Absence of light perception usually indicates either GCA or ophthalmic artery occlusion
DD of CRAO:single or multiple branch retinal artery occlusion,cilioretinal artery occlusion,severe commotio retina,necrotizing herpetic retinitis
#31 Within first few minutes to hours-fundus may appear normal
FIG 1. 3 hour after an attack of CRAO ,retinal whitening is very subtle and retinal vessels appears normal
FIG 2. Box-carring or segmentation of the blood column of both the arteries and veins occurring secondary to separation of blood serum from erythrocytes in a stacked or rouleaux formation
FIG 3. The same eye 24 hours later intense retinal whitening with a cherry-red spot is present. Note the interruption in the blood column of the retinal arteries.
FIG 4.Chronic central retinal artery occlusion in the left eye. Note the optic disc pallor and arterial attenuation
#32 In fresh CRAO residual circulation is almost always present inFFA
GCA causes thrombosis of the common trunk of Post.ciliary artery & CRA arising from the ophthalmic artery
No reflow phenomenon-if there is restoration of circulation in the CRA, thickest part of the macular region do not fill,because of compression of retinal capillaries by the surrounding swollen superficial retinal tissue
.in some cases, despite the CRAO, a small amount of blood may still reach the retina through alternative pathways, such as:Choroidal circulation: The retina also receives some blood supply from the choroid, a vascular layer beneath the retina.
Anastomoses: In some individuals, small connections (anastomoses) between the retinal and choroidal circulation may allow some blood flow to bypass the blockage.
#33 Fig 1 : FFA of the right eye showing a delay in the arterial filling in CRAO at 32 s, 1 m 40 s, 3 min 44 s, and 5 min 35 s.
Fig 2 = Fluorescein angiography at 38 s demonstrates filling of the cilioretinal artery and delayed retinal arterial filling cilioretinal artery will fill during early phase,delayed retinal filiing
Hypofluorescence at involved area late leakage of neovascularization
#34 Fig 1 :Optical coherence tomography demonstrates hyper-reflectivity of the inner retinal layers.
HYPOREFLECTIVE outer retinal layers and shadowing effect due to overlying edema consistent with Central Retinal Artery Occlusion, increased Parafoveal Thickness and Hyporeflective outer Retinal Layers.
Fig2 :Optical coherence tomography image of chronic central retinal artery occlusion in the left eye. Diffuse inner retinal atrophy is appreciated along with outer retinal involvement in the perifoveal macula
Optical intensity ratio (inner retinal layer divided by that of photoreceptor,RPE) correlates with visual outcomes after CRAO
More hyperreflectivity—more ischemia—poor perfusion—poor visual outcomes
#35 ocular Coherence Tomography Angiography (OCTA) (6×6 scan size) shows Disruption of the Superficial Retinal Plexus more in the Nasal Side of the Macula, less Disruption in Deep Retinal Plexus, Hyperfluorescence at the Fovea surrounded by Ischemia in the Choriocapillaris Slap
ACUTE=marked disruption of SPC & DCP,decreased vascular perfusion more in SCP THAN DCP
CHRONIC/LATE=restoration of DCP flow in a patient with cilioretinal artery sparing & decreased flow in the radial peripapillary plexus
#36 Visual field=central scotoma with initial peripheral field defect
Negative waveform from white stimulus
Eventually ,some recovery of visual fields can occur especially in NA-CRAO
Central defect may persist,but peripheral field defect can recover
ERG=B wave reduced while A wave preserved or minimally reduced,studies have correlated B Wave amplitude,B/A ratio & phNR with degree of ischemia & possibility of visual recovery
#37 TEE detected cardiac or thoracic aortic pathologies in 72% of patients with retinal artery occlusion
#40 Ocular massage using a three-mirror contact lens (allows direct artery visualization). The aim is to mechanically collapse the arterial lumen and cause prompt changes in arterial f low, improving perfusion and potentially dislodging an embolus or thrombus. One described method consists of posi tive pressure for 10–15 seconds followed by release, continued for 3–5 minutes.
Self-massage through closed eyelids can be continued by the patient.THIS WILL CAUSE GRADIENTS IN INTRAOCULAR PRESSURE CAUSING A REFLEXIVE ARTERIAL DILATION AS WELL AS INCREASED BLOOD FLOW THROUGH THE ARTERIES THAT HELP TO DISLODGE THE EMBOLUS
BUT IF THERE IS OCULAR SURGERY CONSULT TO THE OPHTHALMOLOGIST FIRST
While four-mirror lenses offer a simultaneous view of the angle, three-mirror lenses are often preferred for their ease of manipulation, surgical access, and comprehensive view of both the angle and the fundus, making them particularly useful for ocular massage and various procedures related to the anterior chamber and retina.
#41 ‘Rebreathing’ into a paper bag in order to elevate blood carbon dioxide and respiratory acidosis has been advocated, as this may promote vasodilatation
Breathing a high oxygen (95%) and carbon dioxide (5%) mixture, ‘carbogen’, has been advocated for a possible dual effect of retarding ischaemia and vasodilatation
Topical apraclonidine 1%, timolol 0.5% and intravenous acetazolamide 500 mg or two 250-mg tablets
to achieve a more sustained lowering of intraocular pressure.
Take 6 to 12 easy, natural breaths, with a small paper bag held over your mouth and nose. Then remove the bag from your nose and mouth and take easy, natural breaths.
Do not use a paper bag if:
You have any heart or lung problems, such as coronary artery disease, asthma, chronic obstructive pulmonary disease (COPD, emphysema), or a history of deep vein thrombosis, stroke, or pulmonary embolism.
HYPERBARIC OXYGEN IN OPHTHALMOLOGY=CRAO,BRAO,optic neuropathy,choroidal neovascularization,DME,DR
#42 Transluminal Nd:YAG laser embolysis/embolectomy(Neodymium:yttrium-aluminum-garnet laser embolectomy)
The neodymium:yttrium-aluminum-garnet laser (1064 nm) is used to lyse the embolus applying power up to 2 mJ.
A variable number of shots of 0.5–1 mJ or higher (to a maximum of 2.4 mJ) are applied directly to the embolus using a fundus contact lens. Embolectomy has been said to occur if the embolus is ejected into the vitreous via a hole in the arteriole. The main complication is subretinal and vitreous haemorrhage in approximately half, which may be curtailed with pressure on the globe
Sublingual isosorbide dinitrate: 10 mg of isosorbide dinitrate causes vasodilation and has been utilized in managing CRAO, although comprehensive studies on its efficacy are currently insufficient
#43 The risk of stroke is relatively high in the first few days following retinal artery occlusion or amaurosis fugax.
IV methylprednisolone: The mainstay of therapy to manage arteritic CRAO caused by giant cell arteritis is 1 g/d for 1 to 3 days. This dose reduces inflammatory causes and retinal edema.
#44 Repeat eye examination in 1 to 4 weeks, checking for neovascularization of the iris/disc/angle/retina (NVI/NVD/NVA/NVE), which develops in up to 20% of patients at a mean of 4 weeks after onset.
#45 Such patient should be warned about the risk of CRAO & evaluated thoroughly for potential risk factors
Possibility of CRAO occurring in the other eye should be explained to the patient.
B=BALANCE LOSS
E= EYE SIGHT CHANGES
F=FACE DROOPING
A=ARM WEAKNESS
S=SPEECH DIFFICULTY
T=TIME TO CALL 911
#47 Study published on American journal of ophthalmology in august 2008
Twenty-eight patients (28 eyes) were included in this study. Final visual acuity was improved three or more lines in nine eyes (32%), stable in 18 (64%), and worse in one eye. Time to treatment < or = 6.5 hours was associated with a better gain of lines of vision (P = .004). Seven of 17 eyes (41%) that received thrombolytic treatment within the first 6.5 hours achieved a final BCVA > or = 20/50, compared to none in the subgroup of patients with onset to treatment >6.5 hours (P = .023). We observed no serious adverse events.
#48 The study was presented at the German Ophthalmological Society
Between 2002 and 2007, 9 centers in Austria and Germany recruited 84 patients (40 received CST, 44 received LIF), and data for 82 patients were analyzed.
Two patients in the CST group (4.3%) and 13 patients in the LIF group (37.1%) had adverse reactions. Because of apparently similar efficacy and the higher rate of adverse reactions in the LIF group, the study was stopped after the first interim analysis at the recommendation of the data and safety monitoring committee.
#49 PVD induction can possibly lead to the release of abnormal adhesion at the level of the CRA. In this case, the hyaloid was quite adherent to the disc and only detached after several attempts.
the active aspiration over the disc may have created a negative suction force that can open the collapsed central retinal artery lumen or dislodge a thrombus. Also, PVD induction may have dislodged a thrombus or an embolus.
Digital subtraction angiography uses X-rays to create images of blood vessels. By subtracting the pre-injection image from the post-injection image (after contrast dye is injected), the blood vessels become more visible.
#56 Branchretinalarteryocclusion in the right eye. (a) Ischemic retinal whitening along superotemporal branch artery. No emboli are visible. (b) Fluorescein angiography demonstrates delayed retinal arterial perfusion superotemporally
#57 Optical coherence tomography (OCT) of acute branch retinal artery occlusion. Infrared reflectance image (left panel) reveals hyporeflectance along the affected superotemporal arteriole and corresponding spectral domain OCT depicts hyper-reflectivity of inner retinal layers
#60 ● DESIGN: Retrospective, observational, consecutive case series.
#63 Cilioretinal obstruction with CRVO (40%)
Generally behaves as a nonischemic central retinal vein obstruction with a good central visual prognosis.
The scotoma from the artery obstruction is usually permanent.
it is hypothesized that some eyes harbor a primary optic disc vasculitis (papillophlebitis) that affects both the arterial and venous circulation
#64 Acute ophthalmic artery occlusion in the left eye. The retina is diffusely pale, and there is no cherry red spot because the choroid is also ischemic. The arteries are very attenuated, and there are a few hemorrhages superiorly.
#65 Acute ophthalmic artery occlusion in the left eye. The retina is diffusely pale, and there is no cherry red spot because the choroid is also ischemic. The arteries are very attenuated, and there are a few hemorrhages superiorly.
#66 Combined Central Retinal Artery Obstruction and Central Retinal Vein Obstruction.
Examination shows a cherry-red spot combined with features of a central retinal vein obstruction, which include dilated, tortuous veins that have retinal hemorrhages in all four quadrants.
Associated systemic or local disease is the rule - collagen vascular disorders, leukemia, orbital trauma, retrobulbar injections, and mucormycosis have been implicated
#67 CAUSES=DM,SYSTEMIC ARTERIAL HYPERTENSION,HIV ASSOCIATED RETINOPATHY,ANEMIA(SEVERE),RADIATION RETINOPATHY,SICKLE CELL RETINOPATHY,CARDIAC EMBOLIC DISEASE,CAROTID ARTERY OBSTRUCTIVE DISEASE,VASCULITIS,COLLAGEN VASCULAR DISEASE,LEUKEMIA,PURTSCHER AND PURTSCHER LIKE RETINOPATHY,GCA
They typically do not cause vision loss, but patients may note small “spots” in their visual fieldhe effect on visual function, including VA loss and VFD, is related to the size and location of the occluded area.
Even if 1 CWS is discovered in the fundus , it should initiate a workup for the most likely under lying etiologies
#68 Spectral-domain optical coherence tomography image showsfocal thickening of the inner retina in the area of the clinically apparent cotton-wool spot
#69 Fig:Color fundus photograph shows patches of middle retinal whitening in the pericentral macula, sparing the peri-arterial retina, with several cotton-wool spots in the peripapillary area and along the vascular arcades.
The lesions may appear only as subtle parafoveal gray- white spots or wedges.
Compared with CWS, the retinal whitening associated with PAMM lesions is more distinct, duller gray- white, less opaque, and deeper in the retina; also, it is not distributed along the NFL
#70 (b) Optical coherence tomography imaging shows hyper reflective bands with a skip pattern, involving predomi nantly the inner nuclear layer. (c) Fluorescein angiography at 55 s after dye injection demonstrated marked delay in retinal arterial filling without evidence for frank arterial occlusion
The lesions may appear only as subtle parafoveal gray- white spots or wedges.
Compared with CWS, the retinal whitening associated with PAMM lesions is more distinct, duller gray- white, less opaque, and deeper in the retina; also, it is not distributed along the NFL
#71 Fundus photo graph of a retinal arterial macroaneurysm with some exudate in the superior macula, resulting from leakage of the lesion, and mild hemorrhage.
#73 Fig;Carotid artery stenosis and ocular implications. Various risk factors contribute to the development of carotid artery stenosis with the consequent development of different aspects of ocular ischemic syndrome and chronic ocular ischemic disease.
main cause of OIS is severe carotid stenosis caused by atherosclerosis leading to reduced perfusion pressure of the central retinal artery . This ischemic insult increases the production of vascular endothelial growth factor (VEGF), resulting in neovascularization and increased vascular permeability . OIS is diagnosed in the presence of amaurosis fugax with or without loss of vision, eye pain, conjunctival or episcleral injection, corneal edema, and ocular signs in the anterior and posterior chamber [
#74 Renal transplant,heart surgeries,spinal surgeries,toxoplasma gondii,dental surgeries
Homocysteine=atherosclerosis by releasing ROS, H2O2 & endothelial cell damage by producing reduced NO & PROTHROMBOTIC STATE DUE TO FACTOR V,X,XII malfunction








































































































![Dry_Eye_Presentation_Final[1].pptx......](https://cdn.slidesharecdn.com/ss_thumbnails/dryeyepresentationfinal1-250516163834-f963ff70-thumbnail.jpg?width=640&height=640&fit=bounds)
























