Downloaded 10 times
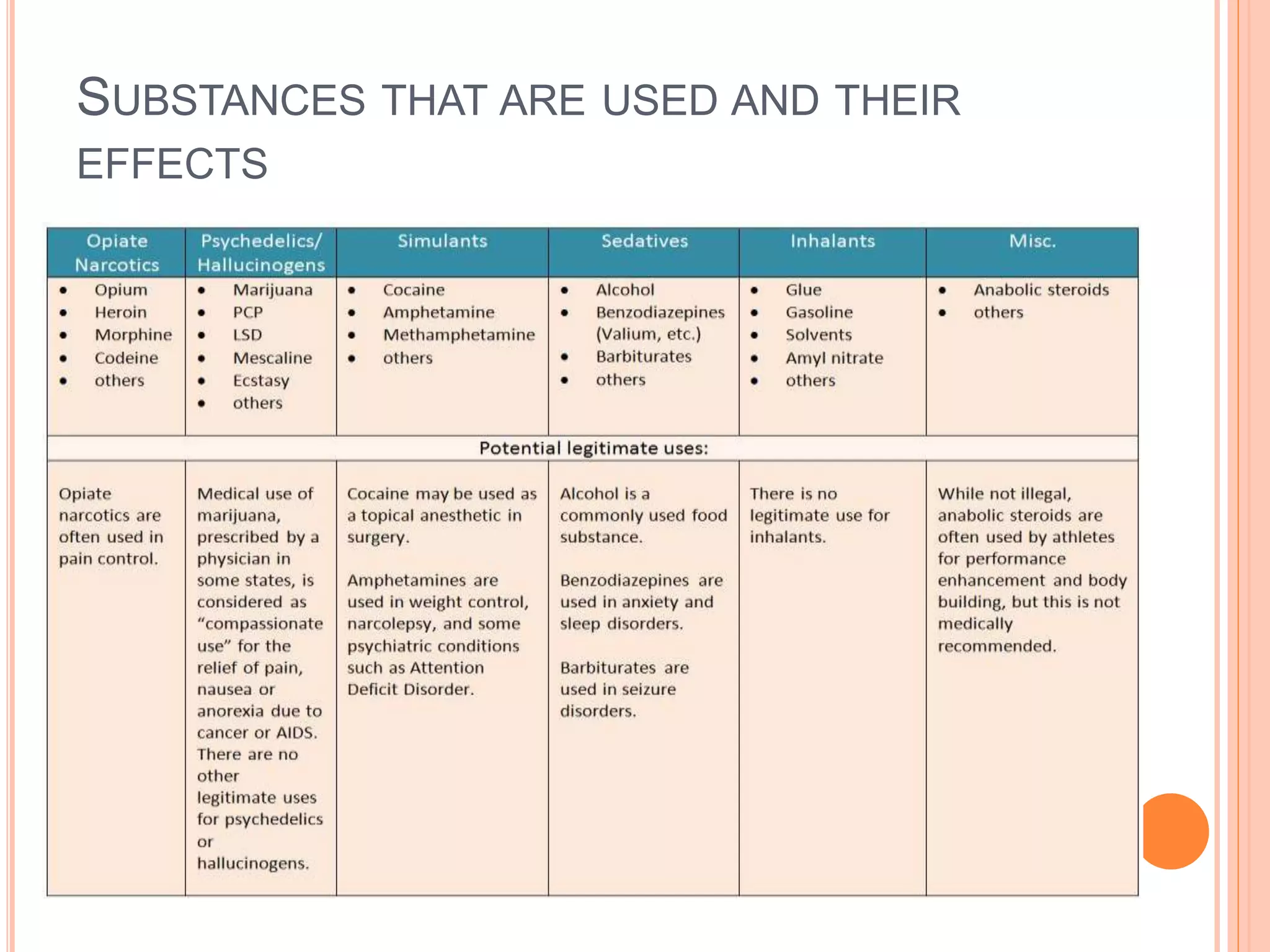
















This document discusses drug abuse, misuse, and control. It begins by defining drug use, misuse, and abuse. It then discusses the definition of rational drug use according to the WHO. Over 50% of drugs are prescribed or used inappropriately. The document outlines various types of drug misuse and their effects. It discusses why people use psychoactive drugs and factors that influence drug choice. Adverse impacts of drug misuse are outlined. The roles of industries, prescribers, patients, and communities in drug misuse are examined. Withdrawal effects and pharmaceutical care approaches are summarized.























































































