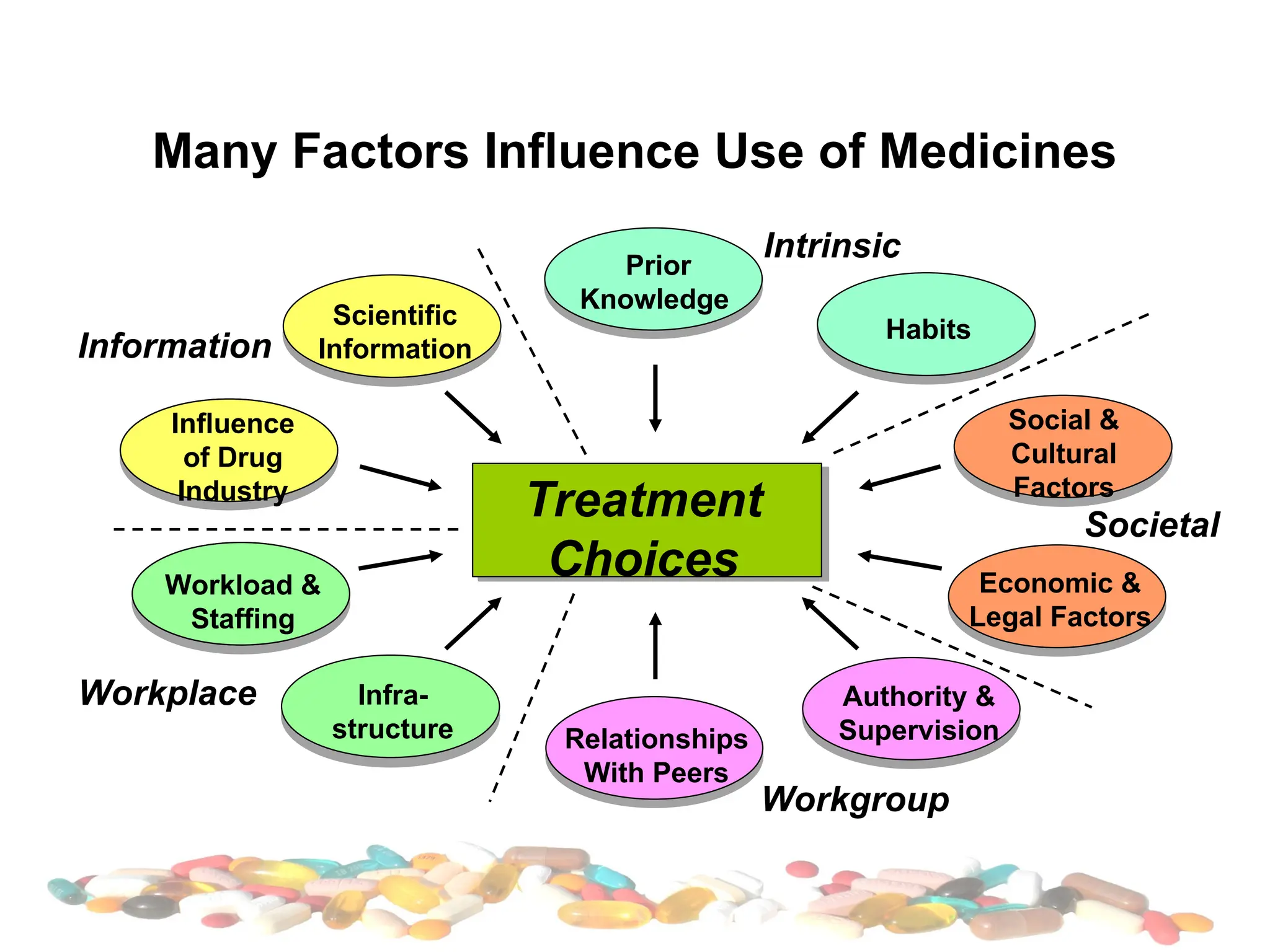
The document discusses the rational use of medications and patient compliance, emphasizing that drugs should be prescribed appropriately, considering efficacy, safety, and patient needs at the lowest cost. It highlights factors leading to irrational use and noncompliance, including lack of information and communication, and outlines steps to improve rational prescribing and adherence. The importance of education, regulatory measures, and the roles of healthcare professionals in promoting rational drug use is also detailed.